Department of Internal Medicine and Liver Research Institute, Seoul National University College of Medicine, Seoul, South Korea.
Department of Internal Medicine, Seoul National University Hospital Healthcare System Gangnam Center, Seoul, South Korea.
Clin Transl Gastroenterol. 2020 Sep;11(9):e00194. doi: 10.14309/ctg.0000000000000194.
We investigated to compare the effect of empirical therapy vs clarithromycin resistance-guided tailored therapy (tailored therapy) for eradication of Helicobacter pylori.
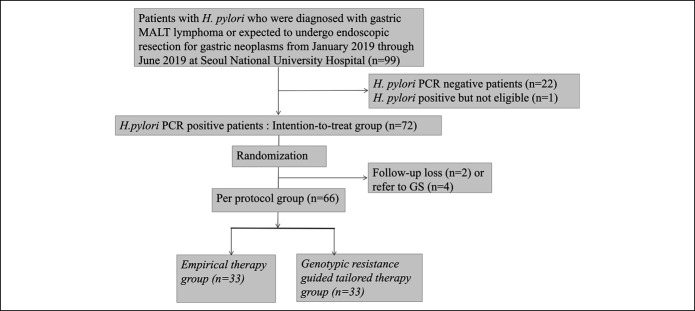
In this prospective, single center, open-label randomized controlled trial, we enrolled 72 patients with H. pylori infection from January 2019 through June 2019 in Korea. The patients were randomly assigned to both groups received empirical (n = 36) or tailored therapy (n = 36). Empirical therapy was defined as triple therapy with esomeprazole, amoxicillin, and clarithromycin for 10 days irrespective of clarithromycin resistance. Tailored therapy was triple or quadruple therapy with esomeprazole, metronidazole, tetracycline, and bismuth for 10 days based on genotype markers of resistance determined by gastric biopsy. Resistance-associated mutations in 23S rRNA were confirmed by multiplex polymerase chain reaction. Eradication status was assessed by C-urea breath test, and the primary outcome was eradication rates.
H. pylori was eradicated in 27 patients (75.0%), given empirical therapy and 32 patients (88.9%) treated with tailored therapy (P = 0.136) in intention-to-treat analysis. In per protocol analysis, the eradication rate was 97.0% and 81.8% in tailoredvs empirical groups (P = 0.046). Although clarithromycin-resistant H. pylori was eradicated in 3/9 (33.3%) with empirical therapy, it was treated in 11/12 (91.7%) with tailored therapy (P = 0.009). There was no difference in compliance between 2 groups. The rate of adverse events of the tailored group was higher than that of the empirical group (P = 0.036) because quadruple therapy had more side effects than those of triple therapy (P = 0.001).
Tailored therapy based on polymerase chain reaction is a good alternative to increase eradication rates in a region of high prevalence of clarithromycin resistance (see Visual Abstract, Supplementary Digital Content 1, http://links.lww.com/CTG/A342).
我们旨在比较经验性治疗与克拉霉素耐药指导下的个体化治疗(个体化治疗)对幽门螺杆菌根除的疗效。
本前瞻性、单中心、开放标签随机对照试验纳入了 2019 年 1 月至 2019 年 6 月期间韩国的 72 例幽门螺杆菌感染患者。将这些患者随机分配至经验性治疗组(n=36)或个体化治疗组(n=36)。经验性治疗定义为不论克拉霉素耐药与否,均采用埃索美拉唑、阿莫西林和克拉霉素三联治疗 10 天。个体化治疗则基于胃活检确定的耐药基因型标志物,采用埃索美拉唑、甲硝唑、四环素和枸橼酸铋四联治疗 10 天。23S rRNA 耐药相关突变通过多重聚合酶链反应确认。通过 C-尿素呼气试验评估根除状态,主要结局为根除率。
在意向性治疗分析中,经验性治疗组 27 例(75.0%)和个体化治疗组 32 例(88.9%)的幽门螺杆菌被根除(P=0.136)。在符合方案分析中,个体化治疗组的根除率为 97.0%,高于经验性治疗组的 81.8%(P=0.046)。虽然经验性治疗组的 3 例(33.3%)克拉霉素耐药的幽门螺杆菌被根除,但在个体化治疗组中,11 例(91.7%)被根除(P=0.009)。两组的依从性无差异。个体化治疗组的不良事件发生率高于经验性治疗组(P=0.036),因为四联疗法比三联疗法的副作用更多(P=0.001)。
基于聚合酶链反应的个体化治疗是在克拉霉素耐药高发地区提高根除率的一种较好的选择(详见视觉摘要,补充数字内容 1,http://links.lww.com/CTG/A342)。