1Medical Research Council Unit The Gambia at LSHTM, Banjul, The Gambia.
2Nigerian Institute of Medical Research (NIMR), Lagos, Nigeria.
Am J Trop Med Hyg. 2020 Dec;103(6):2208-2216. doi: 10.4269/ajtmh.20-0593. Epub 2020 Oct 22.
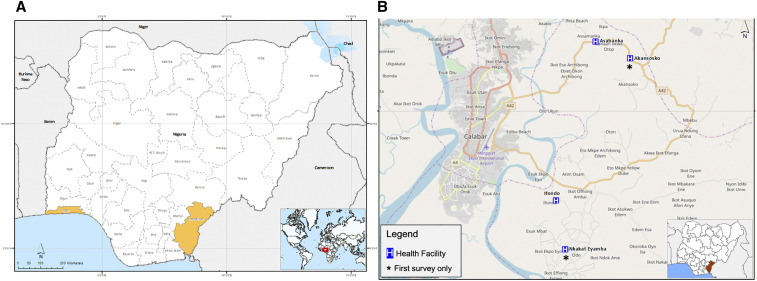
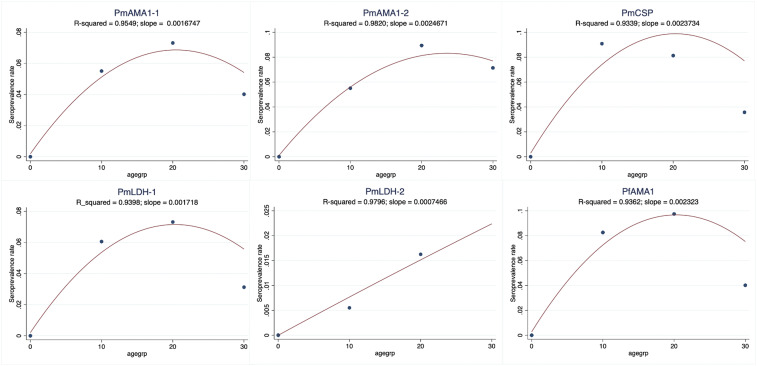
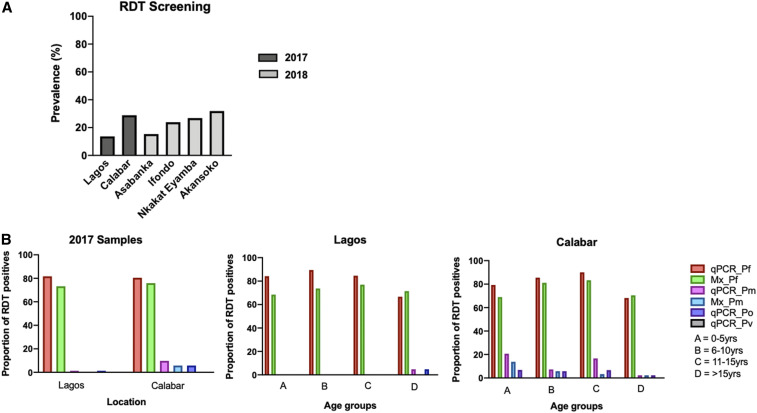
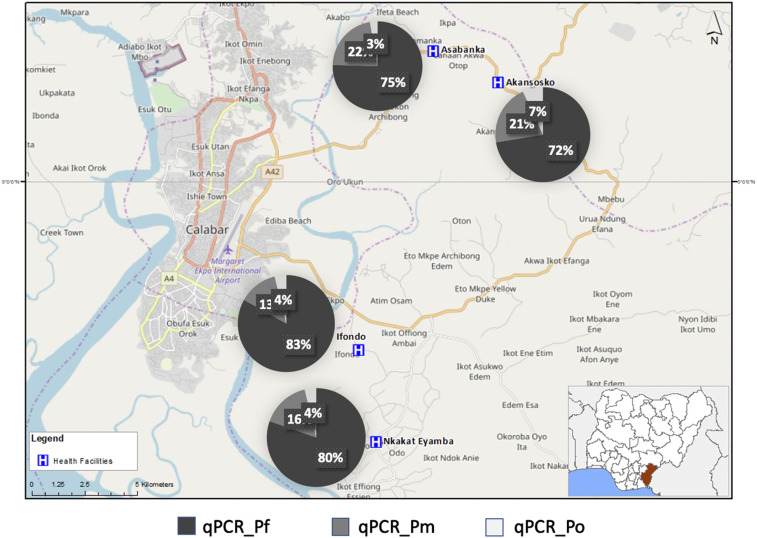
Although continues to be the main target for malaria elimination, other species persist in Africa. Their clinical diagnosis is uncommon, whereas rapid diagnostic tests (RDTs), the most widely used malaria diagnostic tools, are only able to distinguish between and non- species, the latter as "pan-species." Blood samples from health facilities were collected in southern Nigeria (Lagos and Calabar) in 2017 (October-December) and Calabar only in 2018 (October-November), and analyzed by several methods, namely, microscopy, quantitative real-time PCR (qPCR), and peptide serology targeting candidate antigens ( apical membrane antigen, . lactose dehydrogenase, and . circumsporozoite surface protein). Both microscopy and qPCR diagnostic approaches detected comparable proportions (∼80%) of all RDT-positive samples infected with the dominant malaria parasite. However, higher proportions of non- species were detected by qPCR than microscopy, 10% against 3% infections for and 3% against 0% for , respectively. No infection was detected. Infection rates for varied between age-groups, with the highest rates in individuals aged > 5 years. -specific seroprevalence rates fluctuated in those aged < 10 years but generally reached the peak around 20 years of age for all peptides. The heterogeneity and rates of these non-falciparum species call for increased specific diagnosis and targeting by elimination strategies.
虽然 仍然是消除疟疾的主要目标,但其他 物种在非洲仍然存在。它们的临床诊断并不常见,而快速诊断测试(RDTs)是最广泛使用的疟疾诊断工具,只能区分 和非- 物种,后者被称为“泛种”。2017 年(10 月至 12 月)在尼日利亚南部(拉各斯和卡拉巴尔)和仅 2018 年(10 月至 11 月)在卡拉巴尔的医疗机构收集了血液样本,并通过几种方法进行了分析,即显微镜检查、定量实时 PCR(qPCR)和针对候选抗原(顶膜抗原、乳酸脱氢酶和环子孢子表面蛋白)的肽血清学。显微镜检查和 qPCR 诊断方法都检测到了与所有 RDT 阳性样本相似比例(约 80%)的主要 疟原虫寄生虫感染。然而,qPCR 检测到的非- 物种比例高于显微镜检查,分别为 10%和 3%,而 和 感染率分别为 3%和 0%。未检测到 感染。感染率因年龄组而异,年龄大于 5 岁的个体感染率最高。-特异性血清阳性率在年龄小于 10 岁的个体中波动,但对于所有肽,总体在 20 岁左右达到峰值。这些非恶性疟原虫物种的异质性和感染率要求加强特异性诊断,并通过消除策略进行针对性治疗。