Norwegian Centre for Violence and Traumatic Stress Studies, Oslo, Norway.
PLoS One. 2020 Nov 4;15(11):e0241194. doi: 10.1371/journal.pone.0241194. eCollection 2020.
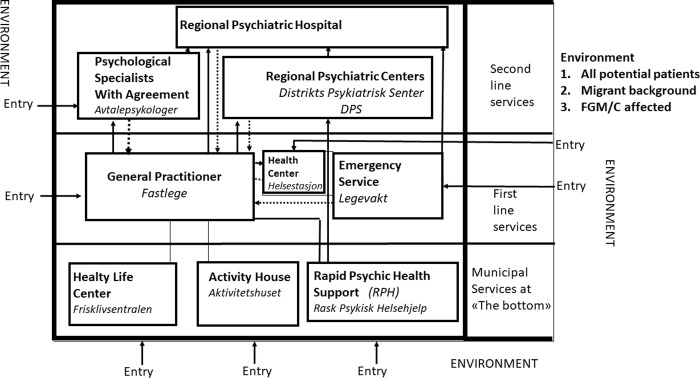
This article explores mental health services in Norway and their availability for women subjected to female genital mutilation/cutting (FGM/C). The article focus on the system of communication and referrals from the perspective of health workers, and aims to identify bottlenecks in the system, what and where they are to be found, and analyze how different mental health services deal with Sub Saharan African (SSA) women in general, but in particular with respect to FGM/C.
The study was conducted in Oslo, Norway, using a qualitative fieldwork research design, with the use of purposeful sampling, and a semi-structural guideline. One hundred interviews were done with general practitioners (GPs), gynecologists, psychologists, psychiatrists, midwives and nurses.
A system analysis is applied using socio-cybernetics as a tool to identify the flow of communication and referrals of patients.
The study shows that borders of subsystems, silencing mechanisms, regulations and "attitudes" of the system can lead to women with SSA background having difficulty getting access to the specialist services. High standards for referral letters, waiting lists, out pushing to the lower levels, insecurities around treatment and deference rules silencing mental health issues during consultancies, have a negative impact on the accessibility of services. Consequences are that mental health problems due to FGM/C are under-investigated, under-referred, and under-treated and a silenced problem within the mental health services for women.
A better integration of subsystems at the specialist level with the GP scheme is necessary, as well as providing competence on FGM/C to the different levels. It is also important to strengthen and integrating the services at the Municipal level and provide information to SSA women about the low threshold services.
本文探讨了挪威的心理健康服务以及这些服务对遭受女性割礼/切割(FGM/C)的女性的可用性。本文从卫生工作者的角度关注沟通和转介系统,旨在确定系统中的瓶颈,找出它们的位置,并分析不同的心理健康服务机构如何总体上处理撒哈拉以南非洲(SSA)女性,特别是针对 FGM/C。
该研究在挪威奥斯陆进行,采用定性实地研究设计,使用有针对性的抽样和半结构化指南。对全科医生、妇科医生、心理学家、精神科医生、助产士和护士进行了 100 次访谈。
应用系统分析,使用社会控制论作为工具,确定患者的沟通和转介流程。
研究表明,子系统的边界、沉默机制、系统的规定和“态度”可能导致 SSA 背景的女性难以获得专科服务。转诊信、等待名单、向下推的高标准、治疗不安和咨询期间尊重规则压制心理健康问题,对服务的可及性产生负面影响。后果是,由于 FGM/C 导致的心理健康问题调查不足、转诊不足和治疗不足,并且是心理健康服务机构中一个被压制的问题。
有必要在专科层面更好地整合子系统与全科医生计划,并向不同层面提供 FGM/C 方面的专业知识。加强和整合市一级的服务,并向 SSA 女性提供关于低门槛服务的信息也很重要。