Gestione Ambulatoriale Politerapie (GAP) Outpatient Clinic, ASST Fatebenefratelli-Sacco University Hospital, Milan, Italy.
Unit of Clinical Pharmacology, ASST Fatebenefratelli-Sacco University Hospital, Milan, Italy.
Drugs Aging. 2020 Dec;37(12):925-933. doi: 10.1007/s40266-020-00812-8. Epub 2020 Nov 5.
Patients hospitalised with severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2; coronavirus 2019 disease (COVID-19)] infection are frequently older with co-morbidities and receiving polypharmacy, all of which are known risk factors for drug-drug interactions (DDIs). The pharmacological burden may be further aggravated by the addition of treatments for COVID-19.
The aim of this study was to assess the risk of potential DDIs upon admission and during hospitalisation in patients with COVID-19 treated at our hospital.
We retrospectively analysed 502 patients with COVID-19 (mean age 61 ± 16 years, range 15-99) treated at our hospital with a proven diagnosis of SARS-CoV-2 infection hospitalised between 21 February and 30 April 2020 and treated with at least two drugs.
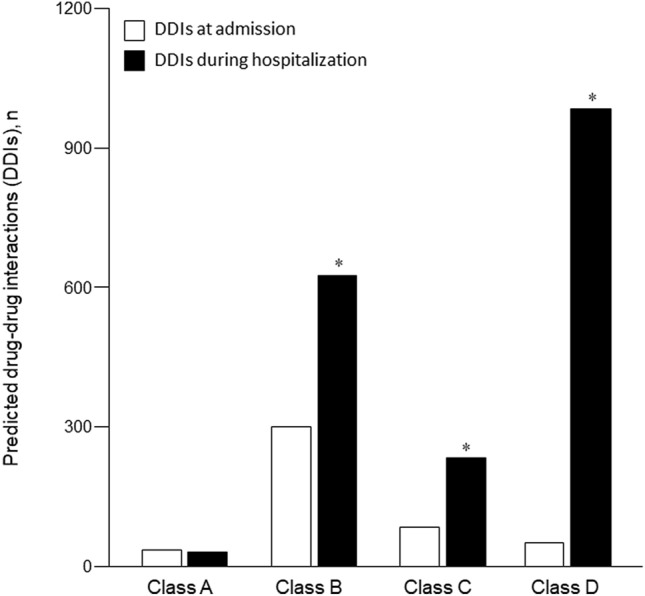
Overall, 68% of our patients with COVID-19 were exposed to at least one potential DDI, and 55% were exposed to at least one potentially severe DDI. The proportion of patients experiencing potentially severe DDIs increased from 22% upon admission to 80% during hospitalisation. Furosemide, amiodarone and quetiapine were the main drivers of potentially severe DDIs upon admission, and hydroxychloroquine and particularly lopinavir/ritonavir were the main drivers during hospitalisation. The majority of potentially severe DDIs carried an increased risk of cardiotoxicity. No potentially severe DDIs were identified in relation to tocilizumab and remdesivir.
Among hospitalised patients with COVID-19, concomitant treatment with lopinavir/ritonavir and hydroxychloroquine led to a dramatic increase in the number of potentially severe DDIs. Given the high risk of cardiotoxicity and the scant and conflicting data concerning their efficacy in treating SARS-CoV-2 infection, the use of lopinavir/ritonavir and hydroxychloroquine in patients with COVID-19 with polypharmacy needs to be carefully considered.
因严重急性呼吸综合征冠状病毒 2[SARS-CoV-2;2019 年冠状病毒病(COVID-19)]感染而住院的患者通常年龄较大,伴有合并症和接受多种药物治疗,这些都是药物-药物相互作用(DDI)的已知危险因素。COVID-19 的治疗可能会进一步加重药物的药理负担。
本研究旨在评估我院收治的 COVID-19 患者入院时和住院期间发生潜在 DDI 的风险。
我们回顾性分析了 502 例于 2020 年 2 月 21 日至 4 月 30 日期间因 SARS-CoV-2 感染住院且至少接受两种药物治疗的 COVID-19 患者(平均年龄 61±16 岁,范围 15-99 岁)。
总体而言,68%的 COVID-19 患者至少发生 1 种潜在 DDI,55%的患者至少发生 1 种潜在严重 DDI。住院期间发生潜在严重 DDI 的患者比例从入院时的 22%上升至 80%。入院时,呋塞米、胺碘酮和喹硫平是潜在严重 DDI 的主要驱动因素,而住院期间,羟氯喹和洛匹那韦/利托那韦是潜在严重 DDI 的主要驱动因素。大多数潜在严重 DDI 增加了心脏毒性风险。托珠单抗和瑞德西韦未发生潜在严重 DDI。
在 COVID-19 住院患者中,洛匹那韦/利托那韦和羟氯喹的联合治疗导致潜在严重 DDI 的数量显著增加。鉴于心脏毒性风险较高,以及关于其治疗 SARS-CoV-2 感染的疗效的有限且相互矛盾的数据,COVID-19 合并症患者使用洛匹那韦/利托那韦和羟氯喹需要仔细考虑。