Sanderson-Cimino Mark, Elman Jeremy A, Tu Xin M, Gross Alden L, Panizzon Matthew S, Gustavson Daniel E, Bondi Mark W, Edmonds Emily C, Eglit Graham M L, Eppig Joel S, Franz Carol E, Jak Amy J, Lyons Michael J, Thomas Kelsey R, Williams McKenna E, Kremen William S
San Diego State University/University of California San Diego Joint Doctoral Program in Clinical Psychology, San Diego, CA, USA.
Center for Behavior Genetics of Aging, University of California, San Diego, La Jolla, CA, USA.
medRxiv. 2020 Nov 5:2020.11.03.20224808. doi: 10.1101/2020.11.03.20224808.
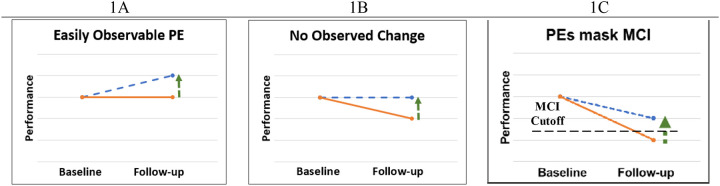
Practice effects on cognitive tests obscure decline, thereby delaying detection of mild cognitive impairment (MCI). This reduces opportunities for slowing Alzheimer's disease progression and can hinder clinical trials. Using a novel method, we assessed the ability of practice-effect-adjusted diagnoses to detect MCI earlier, and tested the validity of these diagnoses based on AD biomarkers.
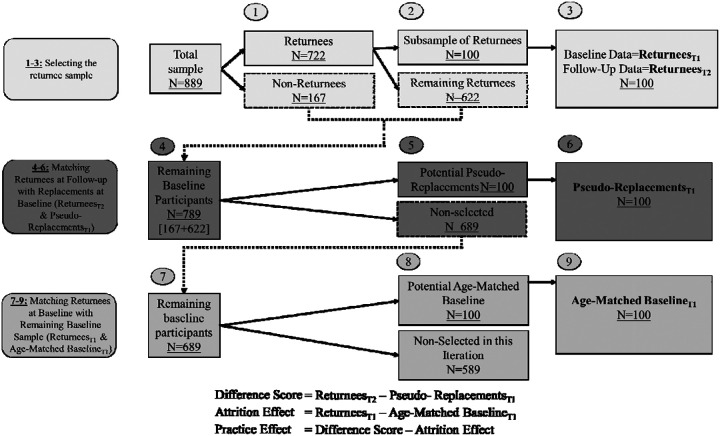
Of 889 Alzheimer's Disease Neuroimaging Initiative participants who were cognitively normal (CN) at baseline, 722 returned at 1-year-follow-up (mean age=74.9±6.8). Practice effects were calculated by comparing returnee scores at follow-up to demographically-matched individuals who had only taken the tests once, with an additional adjustment for attrition effects. Practice effects for each test were subtracted from follow-up scores. The lower scores put additional individuals below the impairment threshold for MCI. CSF amyloid-beta, phosphorylated tau, and total tau were measured at baseline and used for criterion validation.
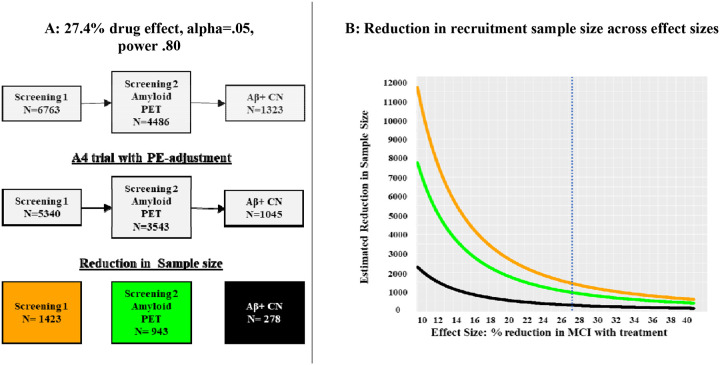
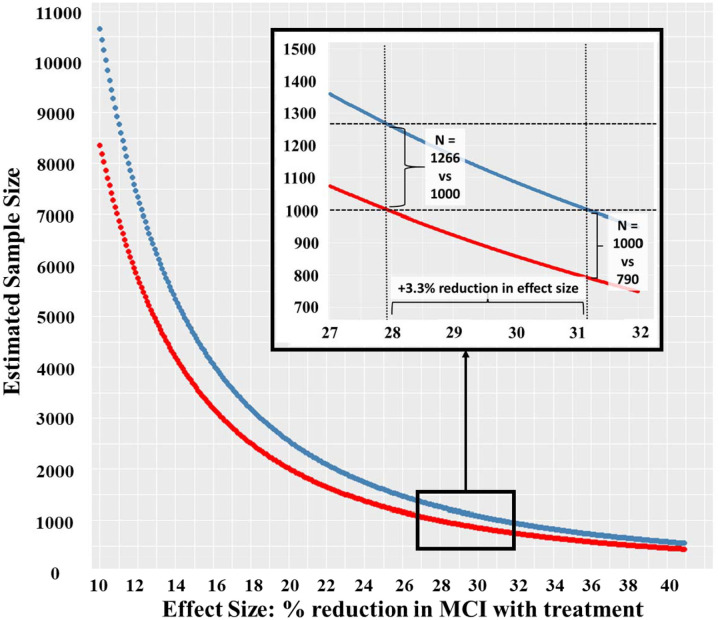
Practice-effect-adjusted scores increased MCI incidence by 26% (p<.001). Adjustment increased proportions of amyloid-positive MCI cases (+20%) and reduced proportions of amyloid-positive CNs (-6%) (ps<.007). With the increased MCI base rate, adjustment for practice effects would reduce the sample size needed for detecting significant drug treatment effects by an average of 21%, which we demonstrate would result in multi-million-dollar savings in a clinical trial.
Adjusting for practice effects on cognitive testing leads to earlier detection of MCI. When MCI is an outcome, this reduces recruitment needed for clinical trials, study duration, staff and participant burden, and can dramatically lower costs. Importantly, biomarker evidence also indicates improved diagnostic accuracy.
认知测试中的练习效应会掩盖衰退,从而延迟轻度认知障碍(MCI)的检测。这减少了减缓阿尔茨海默病进展的机会,并可能阻碍临床试验。我们使用一种新方法评估了经练习效应调整后的诊断更早检测MCI的能力,并基于AD生物标志物测试了这些诊断的有效性。
在889名阿尔茨海默病神经影像学计划参与者中,722名在基线时认知正常(CN),他们在1年随访时返回(平均年龄=74.9±6.8)。通过将随访时返回者的分数与仅进行过一次测试的人口统计学匹配个体的分数进行比较来计算练习效应,并对损耗效应进行额外调整。从随访分数中减去每项测试的练习效应。较低的分数使更多个体低于MCI的损伤阈值。在基线时测量脑脊液淀粉样蛋白-β、磷酸化tau蛋白和总tau蛋白,并用于标准验证。
经练习效应调整后的分数使MCI发病率增加了26%(p<0.001)。调整增加了淀粉样蛋白阳性MCI病例的比例(+20%),并降低了淀粉样蛋白阳性CNs的比例(-6%)(p<0.007)。随着MCI基础率的增加,对练习效应进行调整将使检测显著药物治疗效果所需的样本量平均减少21%,我们证明这将在临床试验中节省数百万美元。
对认知测试中的练习效应进行调整可导致更早检测MCI。当MCI作为一个结果时,这减少了临床试验所需的招募人数、研究持续时间、工作人员和参与者负担,并可显著降低成本。重要的是,生物标志物证据也表明诊断准确性有所提高。