Sentara Heart Hospital, Eastern Virginia Medical School, 600 Gresham Drive, Norfolk, VA, 23507, USA.
Eastern Virginia Medical School, Norfolk, VA, USA.
Curr Heart Fail Rep. 2020 Dec;17(6):333-340. doi: 10.1007/s11897-020-00496-6. Epub 2020 Nov 14.
With improvements in cardiovascular care, and routine percutaneous coronary intervention for ST elevation myocardial infarction, more patients are surviving following acute coronary syndromes. However, a minority of patients develop cardiogenic shock which results in approximately 50% 30-day mortality. There are various ways to classify cardiogenic shock, and much has been written about this topic in recent years. This review will examine recent developments and put them in context.
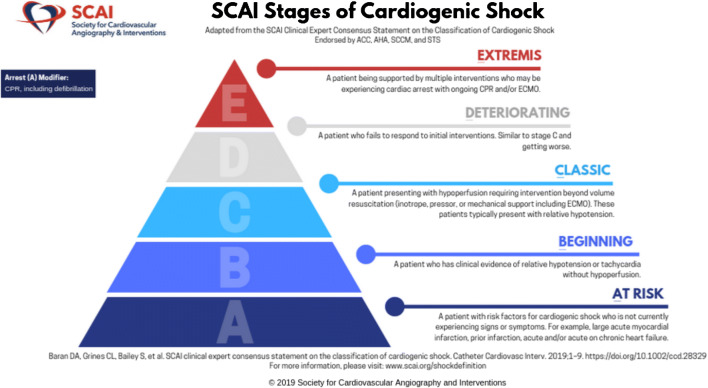
The large randomized trials of cardiogenic shock treatments such as the IABP-SHOCK II trial used a clinical definition of shock including hypotension (systolic blood pressure of 90 mmHg or less, or requirement of vasopressors to maintain such a blood pressure), as well as hypoperfusion. However, while this defines a minimum standard to define cardiogenic shock, it does not distinguish between a patient on a single vasoconstrictor and one who is on multiple high dose infusions or one on extracorporeal membrane oxygenation. The Society for Cardiac Angiography and Intervention recently published an expert consensus statement defining stages of cardiogenic shock, from at risk to beginning, classic, deteriorating, and extremis cardiogenic shock stages. The simple framework has been validated rapidly in multiple populations including the intensive care unit, a post-myocardial infarction population, an out of hospital cardiac arrest population, and most recently in a multicenter shock collaborative, Classification is fundamental to understanding a disease state, and crafting solutions to improve outcomes. The last 20 years has witnessed an explosion of percutaneous mechanical circulatory support devices of increasing sophistication and capability, and yet there has been little progress in improving outcomes of cardiogenic shock. Hopefully, the next 20 years will see massive advances in understanding of the complexities of the various stages of cardiogenic shock. With such knowledge, it is likely that targeted treatments will be developed and the mortality of this disease will finally plummet.
随着心血管治疗的改善以及常规经皮冠状动脉介入治疗 ST 段抬高型心肌梗死,越来越多的急性冠状动脉综合征患者存活下来。然而,少数患者会发展为心源性休克,导致约 50%的患者在 30 天内死亡。心源性休克有多种分类方法,近年来对此进行了大量研究。本综述将探讨最近的进展并进行分析。
大规模随机临床试验,如 IABP-SHOCK II 试验,采用临床定义的休克标准,包括低血压(收缩压 90mmHg 以下或需要升压药维持如此血压)和灌注不足。然而,虽然这定义了定义心源性休克的最低标准,但它并不能区分仅使用一种血管收缩剂的患者与使用多种高剂量输注或体外膜氧合的患者。心血管造影和介入学会最近发布了一份专家共识声明,定义了心源性休克的分期,从高危期到开始期、经典期、恶化期和极期。这个简单的框架已经在多个人群中迅速得到验证,包括重症监护病房、心肌梗死后人群、院外心脏骤停人群,最近还在多中心休克协作研究中得到验证。分类是理解疾病状态和制定改善预后的解决方案的基础。过去 20 年见证了越来越复杂和强大的经皮机械循环支持设备的爆炸式发展,但心源性休克的预后改善却很少。希望未来 20 年能在理解心源性休克的各个阶段的复杂性方面取得重大进展。有了这些知识,很可能会开发出针对特定疾病的治疗方法,从而使这种疾病的死亡率最终大幅下降。