Clinical, cognitive and computational neuroimaging laboratory (C3NL), Department of Brain Sciences, Faculty of Medicine, Imperial College London, London, W12 0NN, UK.
UK Dementia Research Institute Care Research and Technology Centre, Imperial College London and the University of Surrey, London, W12 0NN UK.
Brain. 2021 Feb 12;144(1):92-113. doi: 10.1093/brain/awaa372.
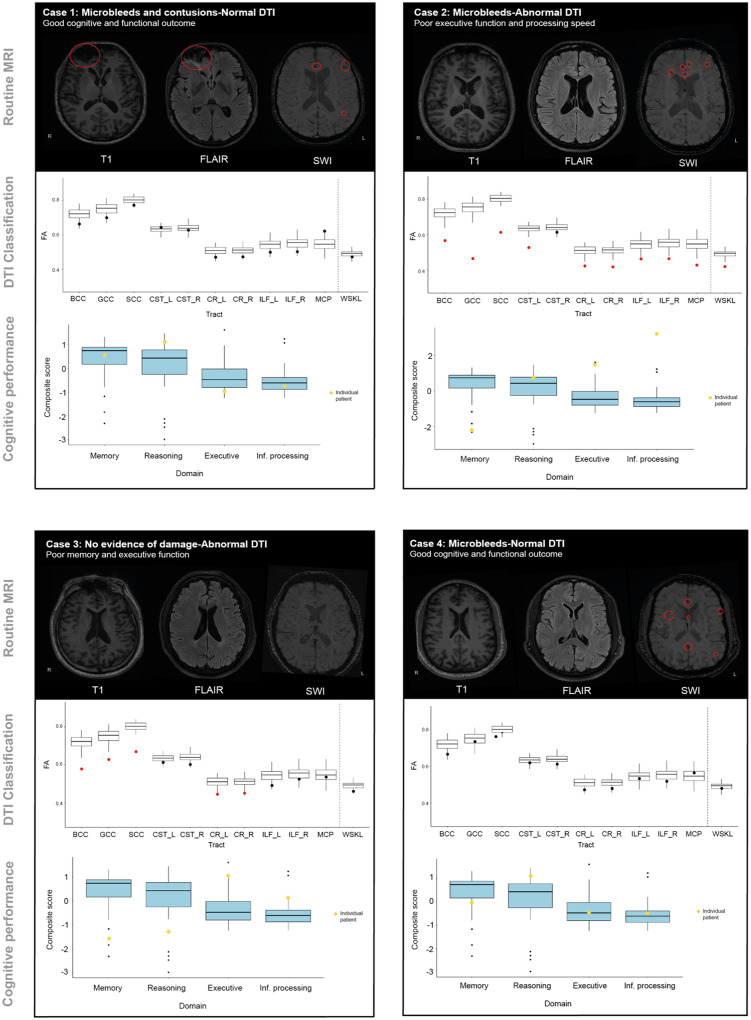
Poor outcomes after traumatic brain injury (TBI) are common yet remain difficult to predict. Diffuse axonal injury is important for outcomes, but its assessment remains limited in the clinical setting. Currently, axonal injury is diagnosed based on clinical presentation, visible damage to the white matter or via surrogate markers of axonal injury such as microbleeds. These do not accurately quantify axonal injury leading to misdiagnosis in a proportion of patients. Diffusion tensor imaging provides a quantitative measure of axonal injury in vivo, with fractional anisotropy often used as a proxy for white matter damage. Diffusion imaging has been widely used in TBI but is not routinely applied clinically. This is in part because robust analysis methods to diagnose axonal injury at the individual level have not yet been developed. Here, we present a pipeline for diffusion imaging analysis designed to accurately assess the presence of axonal injury in large white matter tracts in individuals. Average fractional anisotropy is calculated from tracts selected on the basis of high test-retest reliability, good anatomical coverage and their association to cognitive and clinical impairments after TBI. We test our pipeline for common methodological issues such as the impact of varying control sample sizes, focal lesions and age-related changes to demonstrate high specificity, sensitivity and test-retest reliability. We assess 92 patients with moderate-severe TBI in the chronic phase (≥6 months post-injury), 25 patients in the subacute phase (10 days to 6 weeks post-injury) with 6-month follow-up and a large control cohort (n = 103). Evidence of axonal injury is identified in 52% of chronic and 28% of subacute patients. Those classified with axonal injury had significantly poorer cognitive and functional outcomes than those without, a difference not seen for focal lesions or microbleeds. Almost a third of patients with unremarkable standard MRIs had evidence of axonal injury, whilst 40% of patients with visible microbleeds had no diffusion evidence of axonal injury. More diffusion abnormality was seen with greater time since injury, across individuals at various chronic injury times and within individuals between subacute and 6-month scans. We provide evidence that this pipeline can be used to diagnose axonal injury in individual patients at subacute and chronic time points, and that diffusion MRI provides a sensitive and complementary measure when compared to susceptibility weighted imaging, which measures diffuse vascular injury. Guidelines for the implementation of this pipeline in a clinical setting are discussed.
创伤性脑损伤 (TBI) 后预后不良较为常见,但仍难以预测。弥漫性轴索损伤对预后很重要,但在临床环境中其评估仍受到限制。目前,轴索损伤是基于临床表现、白质的可见损伤或轴索损伤的替代标志物(如微出血)来诊断的。这些方法并不能准确地量化轴索损伤,导致一部分患者误诊。弥散张量成像可提供体内轴索损伤的定量测量,各向异性分数常被用作白质损伤的替代物。弥散成像已广泛应用于 TBI 中,但并未常规应用于临床。这在一定程度上是因为尚未开发出用于个体水平诊断轴索损伤的稳健分析方法。在这里,我们提出了一种弥散成像分析的工作流程,旨在准确评估个体中大的白质束中轴索损伤的存在。基于高测试-重测可靠性、良好的解剖学覆盖范围以及它们与 TBI 后认知和临床障碍的相关性,选择轨迹来计算平均各向异性分数。我们测试了我们的工作流程是否存在常见的方法学问题,如不同对照组样本量、局灶性病变和与年龄相关的变化的影响,以证明其具有高特异性、敏感性和测试-重测可靠性。我们评估了 92 名处于慢性期(受伤后≥6 个月)的中重度 TBI 患者、25 名亚急性期(受伤后 10 天至 6 周)患者和一个大的对照组(n=103),并进行了 6 个月的随访。在慢性期和亚急性期患者中分别有 52%和 28%的患者发现了轴索损伤的证据。与没有轴索损伤的患者相比,被分类为有轴索损伤的患者认知和功能结局明显更差,而局灶性病变或微出血的患者则没有这种差异。将近三分之一的 MRI 未见明显异常的患者有轴索损伤的证据,而 40%有可见微出血的患者则没有弥散异常的证据。随着时间的推移,个体在不同的慢性损伤时间点以及个体在亚急性期和 6 个月扫描之间,弥散异常的情况更明显。我们提供的证据表明,该工作流程可用于在亚急性期和慢性期诊断个体患者的轴索损伤,与测量弥漫性血管损伤的磁敏感加权成像相比,弥散 MRI 是一种更敏感和互补的测量方法。讨论了在临床环境中实施该工作流程的指南。