Le Grange Daniel, Eckhardt Sarah, Dalle Grave Riccardo, Crosby Ross D, Peterson Carol B, Keery Helene, Lesser Julie, Martell Carolyn
University of California, San Francisco, San Francisco, CA, USA.
The University of Chicago, Chicago, IL, USA (Emeritus).
Psychol Med. 2020 Dec 3;52(13):1-11. doi: 10.1017/S0033291720004407.
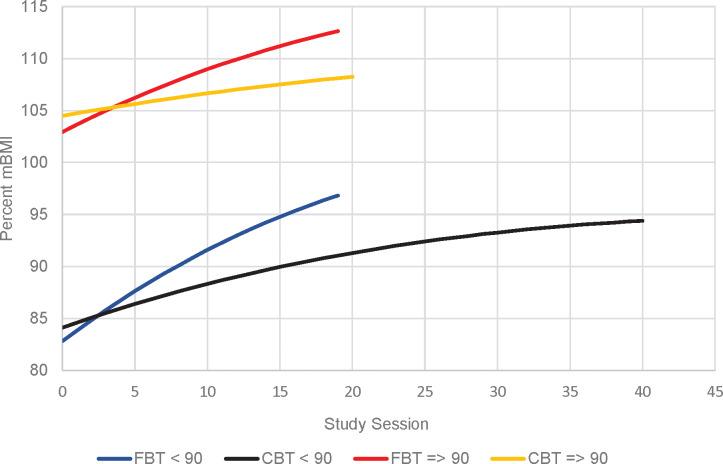
Family-based treatment (FBT) is an efficacious intervention for adolescents with an eating disorder. Evaluated to a lesser degree among adolescents, enhanced cognitive-behavior therapy (CBT-E) has shown promising results. This study compared the relative effectiveness of FBT and CBT-E, and as per manualized CBT-E, the sample was divided into a lower weight [<90% median body mass index (mBMI)], and higher weight cohort (⩾90%mBMI).
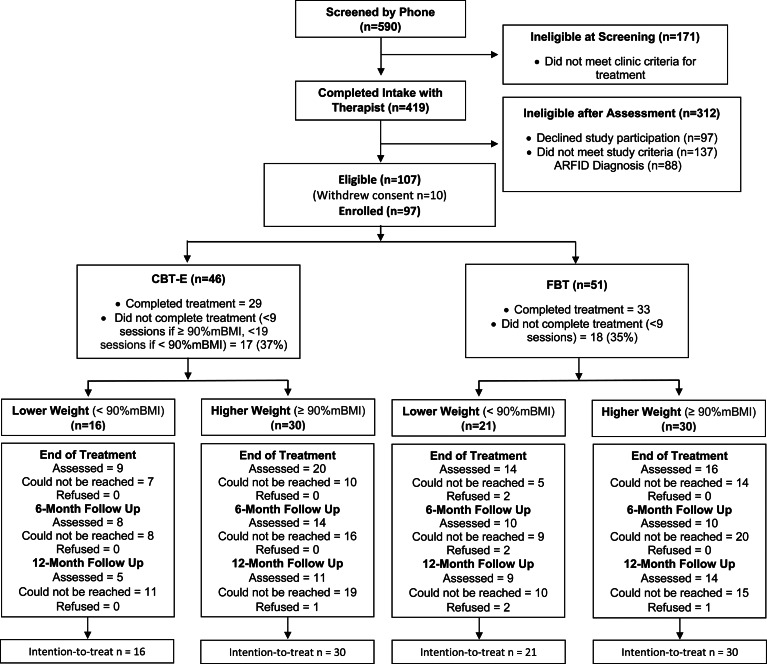
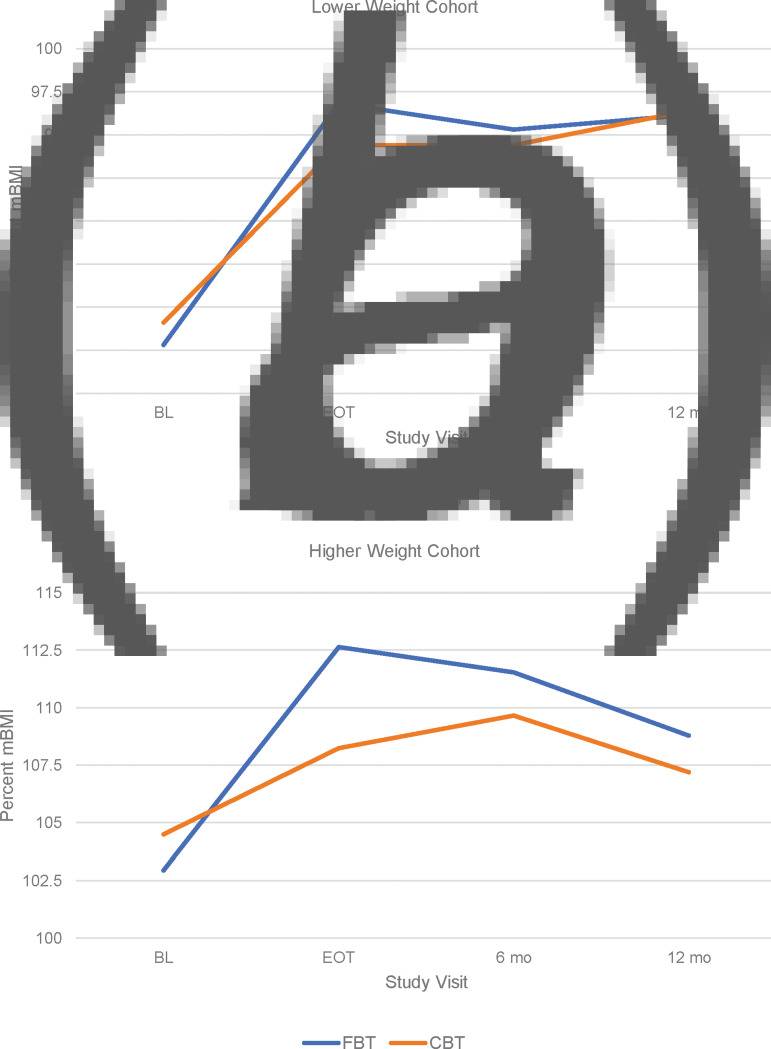
Participants (N = 97) aged 12-18 years, with a DSM-5 eating disorder diagnosis (largely restrictive, excluding Avoidant Restrictive Food Intake Disorder), and their parents, chose between FBT and CBT-E. Assessments were administered at baseline, end-of-treatment (EOT), and follow-up (6 and 12 months). Treatment comprised of 20 sessions over 6 months, except for the lower weight cohort where CBT-E comprised 40 sessions over 9-12 months. Primary outcomes were slope of weight gain and change in Eating Disorder Examination (EDE) Global Score at EOT.
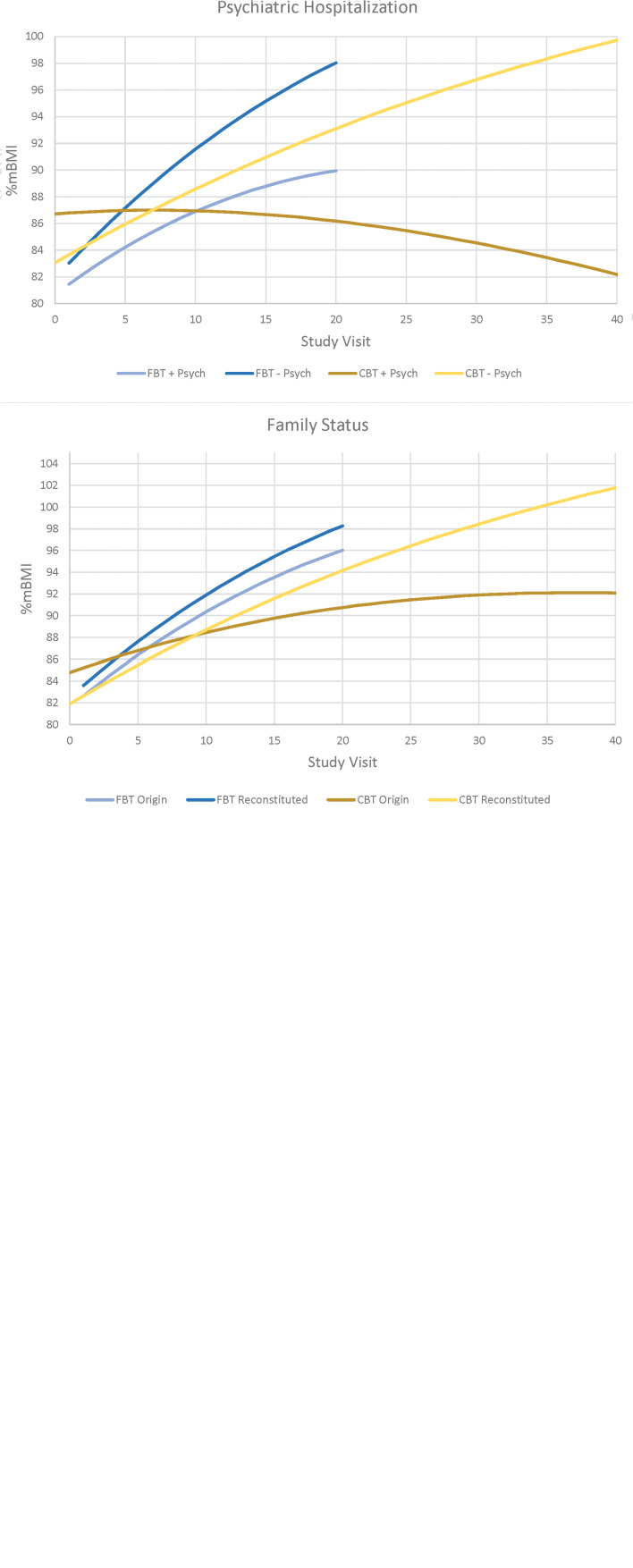
Slope of weight gain at EOT was significantly higher for FBT than for CBT-E (lower weight, est. = 0.597, s.e. = 0.096, p < 0.001; higher weight, est. = 0.495, s.e. = 0.83, p < 0.001), but not at follow-up. There were no differences in the EDE Global Score or most secondary outcome measures at any time-point. Several baseline variables emerged as potential treatment effect moderators at EOT. Choosing between FBT and CBT-E resulted in older and less well participants opting for CBT-E.
Results underscore the efficiency of FBT to facilitate weight gain among underweight adolescents. FBT and CBT-E achieved similar outcomes in other domains assessed, making CBT-E a viable treatment for adolescents with an eating disorder.
Treatment Outcome in Eating Disorders; https://clinicaltrials.gov/; NCT03599921.
基于家庭的治疗(FBT)是一种治疗青少年饮食失调的有效干预措施。在青少年中评估程度较低的强化认知行为疗法(CBT-E)已显示出有前景的结果。本研究比较了FBT和CBT-E的相对有效性,并且根据标准化的CBT-E,将样本分为体重较低组(<90%中位数体重指数[mBMI])和体重较高组(⩾90%mBMI)。
年龄在12 - 18岁、患有DSM-5饮食失调诊断(主要为限制性,不包括回避性限制性食物摄入障碍)的参与者及其父母,在FBT和CBT-E之间进行选择。在基线、治疗结束时(EOT)和随访(6个月和12个月)时进行评估。治疗包括在6个月内进行20次治疗,体重较低组的CBT-E则在9 - 12个月内进行40次治疗。主要结局是治疗结束时体重增加的斜率和饮食失调检查(EDE)全球评分的变化。
治疗结束时,FBT的体重增加斜率显著高于CBT-E(体重较低组,估计值 = 0.597,标准误 = 0.096,p < 0.001;体重较高组,估计值 = 0.495,标准误 = 0.83,p < 0.001),但在随访时并非如此。在任何时间点,EDE全球评分或大多数次要结局指标均无差异。几个基线变量在治疗结束时成为潜在的治疗效果调节因素。在FBT和CBT-E之间进行选择导致年龄较大且状况较差的参与者选择CBT-E。
结果强调了FBT在促进体重过轻青少年体重增加方面的有效性。FBT和CBT-E在评估的其他领域取得了相似的结果,使CBT-E成为治疗青少年饮食失调的一种可行疗法。
饮食失调的治疗结果;https://clinicaltrials.gov/;NCT03599921。