Headache and Facial Pain Group, UCL Queen Square Institute of Neurology and National Hospital for Neurology and Neurosurgery, London, UK.
Biostatistician, Education Unit, UCL Queen Square Institute of Neurology, London UK.
Brain. 2020 Dec 1;143(12):3619-3628. doi: 10.1093/brain/awaa331.
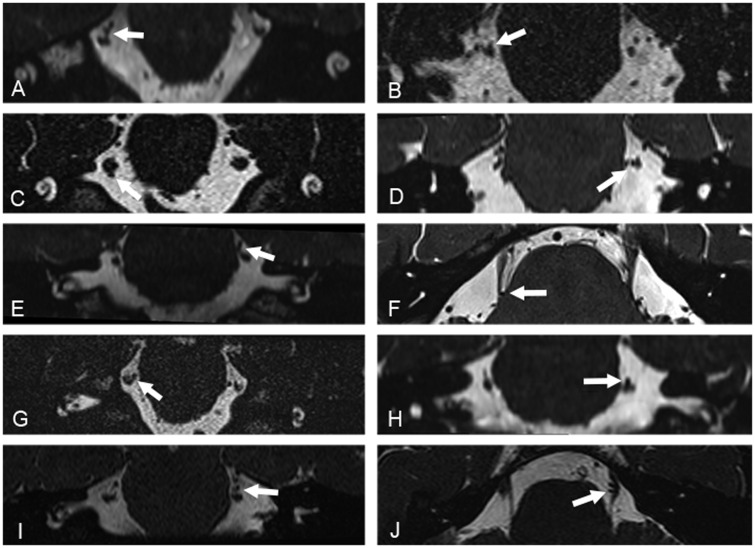
Emerging data-points towards a possible aetiological and therapeutic relevance of trigeminal neurovascular contact in short lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and perhaps in short lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA). We aimed to assess the prevalence and significance of trigeminal neurovascular contact in a large cohort of consecutive SUNCT and SUNA patients and evaluate the radiological differences between them. The standard imaging protocol included high spatial and nerve-cistern contrast resolution imaging acquisitions of the cisternal segments of the trigeminal nerves and vessels. MRI studies were evaluated blindly by two expert evaluators and graded according to the presence, location and degree of neurovascular contact. The degree of contact was graded as with or without morphological changes. Neurovascular contact with morphological changes was defined as contact with distortion and/or atrophy. A total of 159 patients (SUNCT = 80; SUNA = 79) were included. A total of 165 symptomatic and 153 asymptomatic trigeminal nerves were analysed. The proportion of neurovascular contact on the symptomatic trigeminal nerves was higher (80.0%) compared to the asymptomatic trigeminal nerves (56.9%). The odds on having neurovascular contact over the symptomatic nerves was significantly higher than on the asymptomatic nerves [odds ratio (OR): 3.03, 95% confidence interval (CI) 1.84-4.99; P < 0.0001]. Neurovascular contact with morphological changes were considerably more prevalent on the symptomatic side (61.4%), compared to the asymptomatic side (31.0%) (OR 4.16, 95% CI 2.46-7.05; P < 0.0001). On symptomatic nerves, neurovascular contact with morphological changes was caused by an artery in 95.0% (n = 77/81). Moreover, the site of contact and the point of contact around the trigeminal root were respectively proximal in 82.7% (67/81) and superior in 59.3% (48/81). No significant radiological differences emerged between SUNCT and SUNA. The multivariate analysis of radiological predictors associated with the symptomatic side, indicated that the presence of neurovascular contact with morphological changes was strongly associated with the side of the pain (OR: 2.80, 95% CI 1.44-5.44; P = 0.002) even when adjusted for diagnoses. Our findings suggest that neurovascular contact with morphological changes is involved in the aetiology of SUNCT and SUNA. Along with a similar clinical phenotype, SUNCT and SUNA also display a similar structural neuroimaging profile, providing further support for the concept that the separation between them should be abandoned. Furthermore, these findings suggest that vascular compression of the trigeminal sensory root, may be a common aetiological factor between SUNCT, SUNA and trigeminal neuralgia thereby further expanding the overlap between these disorders.
新出现的数据表明,三叉神经血管接触在短暂单侧丛集性头痛发作伴结膜充血和流泪(SUNCT)和短暂单侧丛集性头痛发作伴颅自主症状(SUNA)中可能具有病因学和治疗学意义。我们旨在评估大量连续 SUNCT 和 SUNA 患者中三叉神经血管接触的患病率和意义,并评估它们之间的放射学差异。标准成像方案包括三叉神经和血管的脑池段的高空间和神经 - 脑池对比分辨率成像采集。MRI 研究由两位专家评估员进行盲法评估,并根据神经血管接触的存在、位置和程度进行分级。接触程度分为有或无形态学变化。具有形态学变化的神经血管接触定义为接触伴有扭曲和/或萎缩。共纳入 159 例患者(SUNCT=80;SUNA=79)。共分析了 165 条有症状和 153 条无症状三叉神经。有症状三叉神经上的神经血管接触比例较高(80.0%),而无症状三叉神经上的神经血管接触比例较低(56.9%)。有症状神经上神经血管接触的可能性明显高于无症状神经[比值比(OR):3.03,95%置信区间(CI)1.84-4.99;P<0.0001]。有形态学变化的神经血管接触在症状侧(61.4%)明显更为常见,而在无症状侧(31.0%)(OR 4.16,95%CI 2.46-7.05;P<0.0001)。在有症状的神经上,95.0%(n=77/81)的神经血管接触是由动脉引起的。此外,接触部位和三叉神经根周围的接触点分别位于近端 82.7%(67/81)和上部 59.3%(48/81)。SUNCT 和 SUNA 之间没有出现明显的放射学差异。与症状侧相关的放射学预测因素的多变量分析表明,有形态学变化的神经血管接触与疼痛侧之间存在很强的相关性(OR:2.80,95%CI 1.44-5.44;P=0.002),即使在调整诊断后也是如此。我们的研究结果表明,具有形态学变化的神经血管接触可能与 SUNCT 和 SUNA 的病因有关。SUNCT 和 SUNA 除了具有相似的临床表型外,还具有相似的结构神经影像学特征,这进一步支持了它们之间的分离应该被摒弃的观点。此外,这些发现表明,三叉神经感觉根的血管压迫可能是 SUNCT、SUNA 和三叉神经痛之间的共同病因,从而进一步扩大了这些疾病之间的重叠。