Headache and Facial Pain Group, UCL Queen Square Institute of Neurology and National Hospital for Neurology and Neurosurgery, London, UK.
Lysholm Department of Neuroradiology, UCL Queen Square Institute of Neurology and National Hospital for Neurology and Neurosurgery, London, UK.
Brain. 2022 Aug 27;145(8):2882-2893. doi: 10.1093/brain/awac109.
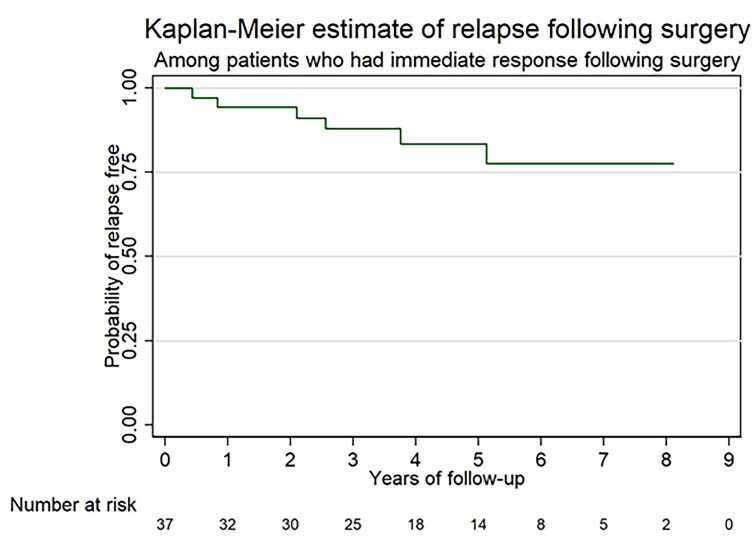
A significant proportion of patients with short-lasting unilateral neuralgiform headache attacks are refractory to medical treatments. Neuroimaging studies have suggested a role for ipsilateral trigeminal neurovascular conflict with morphological changes in the pathophysiology of this disorder. We present the outcome of an uncontrolled open-label prospective single-centre study conducted between 2012 and 2020, to evaluate the efficacy and safety of trigeminal microvascular decompression in refractory chronic short-lasting unilateral neuralgiform headache attacks with MRI evidence of trigeminal neurovascular conflict ipsilateral to the pain side. Primary endpoint was the proportion of patients who achieved an 'excellent response', defined as 90-100% weekly reduction in attack frequency, or 'good response', defined as a reduction in weekly headache attack frequency between 75% and 89% at final follow-up, compared to baseline. These patients were defined as responders. The study group consisted of 47 patients, of whom 31 had short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing, and 16 had short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (25 females, mean age ± SD 55.2 years ± 14.8). Participants failed to respond or tolerate a mean of 8.1 (±2.7) preventive treatments pre-surgery. MRI of the trigeminal nerves (n = 47 patients, n = 50 symptomatic trigeminal nerves) demonstrated ipsilateral neurovascular conflict with morphological changes in 39/50 (78.0%) symptomatic nerves and without morphological changes in 11/50 (22.0%) symptomatic nerves. Postoperatively, 37/47 (78.7%) patients obtained either an excellent or a good response. Ten patients (21.3%, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing = 7 and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms = 3) reported no postoperative improvement. The mean post-surgery follow-up was 57.4 ± 24.3 months (range 11-96 months). At final follow-up, 31 patients (66.0%) were excellent/good responders. Six patients experienced a recurrence of headache symptoms. There was no statistically significant difference between short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing and short-lasting unilateral neuralgiform headache attacks in the response to surgery (P = 0.463). Responders at the last follow-up were, however, more likely to not have interictal pain (77.42% versus 22.58%, P = 0.021) and to show morphological changes on the MRI (78.38% versus 21.62%, P = 0.001). The latter outcome was confirmed in the Kaplan-Meyer analysis, where patients with no morphological changes were more likely to relapse overtime compared to those with morphological changes (P = 0.0001). All but one patient, who obtained an excellent response without relapse, discontinued their preventive medications. Twenty-two post-surgery adverse events occurred in 18 patients (46.8%) but no mortality or severe neurological deficit was seen. Trigeminal microvascular decompression may be a safe and effective long-term treatment for patients suffering short-lasting unilateral neuralgiform headache attacks with MRI evidence of neurovascular conflict with morphological changes.
相当比例的短暂单侧丛集性头痛发作患者对药物治疗无反应。神经影像学研究表明,同侧三叉神经血管冲突与这种疾病的病理生理学中的形态变化有关。我们报告了 2012 年至 2020 年期间进行的一项非对照开放标签前瞻性单中心研究的结果,以评估三叉神经微血管减压术治疗有 MRI 证据显示同侧三叉神经血管冲突的难治性慢性短暂单侧丛集性头痛发作的疗效和安全性。主要终点是达到“优秀反应”的患者比例,定义为每周头痛发作频率减少 90-100%,或“良好反应”,定义为与基线相比,每周头痛发作频率减少 75%-89%。这些患者被定义为有反应者。研究组包括 47 名患者,其中 31 名患有伴有结膜充血和流泪的短暂单侧丛集性头痛发作,16 名患有伴有颅自主神经症状的短暂单侧丛集性头痛发作(25 名女性,平均年龄 55.2 ± 14.8 岁)。参与者在手术前平均未能对 8.1(±2.7)种预防性治疗方法产生反应或耐受。对 47 名患者(n=50 条有症状的三叉神经)的三叉神经 MRI 显示,39/50(78.0%)有症状的神经存在同侧神经血管冲突和形态变化,11/50(22.0%)有症状的神经无形态变化。术后,37/47(78.7%)名患者获得了优秀或良好的反应。10 名患者(21.3%,伴有结膜充血和流泪的短暂单侧丛集性头痛发作=7 例,伴有颅自主神经症状的短暂单侧丛集性头痛发作=3 例)报告术后无改善。术后平均随访时间为 57.4 ± 24.3 个月(范围 11-96 个月)。在最后一次随访时,31 名患者(66.0%)为优秀/良好反应者。6 名患者出现头痛症状复发。在手术反应方面,伴有结膜充血和流泪的短暂单侧丛集性头痛发作与短暂单侧丛集性头痛发作之间无统计学差异(P=0.463)。然而,在最后一次随访时有反应的患者更有可能没有发作间期疼痛(77.42%对 22.58%,P=0.021),并且 MRI 上显示形态变化(78.38%对 21.62%,P=0.001)。在 Kaplan-Meier 分析中证实了这一结果,其中没有形态变化的患者在随访期间更有可能复发,而有形态变化的患者则较少复发(P=0.0001)。除了一名没有复发且获得优秀反应的患者外,其余患者均停止了预防性药物治疗。18 名患者(46.8%)发生了 22 例术后不良事件,但无死亡或严重神经功能缺损。三叉神经微血管减压术可能是一种安全有效的长期治疗方法,适用于 MRI 显示有神经血管冲突伴形态变化的短暂单侧丛集性头痛发作患者。