Department of Population Medicine, University of Guelph, Guelph, ON, Canada.
Food-Borne Disease and Antimicrobial Resistance Surveillance Division, Centre of Food-borne Environmental and Zoonotic Infectious Diseases, Public Health Agency of Canada, Guelph, ON, Canada.
Antimicrob Resist Infect Control. 2020 Dec 10;9(1):200. doi: 10.1186/s13756-020-00863-x.
Assessment of the burden of disease due to antimicrobial-resistant Escherichia coli infections facilitates understanding the scale of the problem and potential impacts, and comparison to other diseases, which allows prioritization of research, surveillance, and funding. Using systematic review and meta-analysis methodology, the objectives were to evaluate whether humans with antimicrobial-resistant E. coli infections experience increases in measures of health or healthcare system burden when compared to susceptible E. coli infections.
Comprehensive literature searches were performed in four primary and seven grey literature databases. Analytic observational studies of human E. coli infections that assessed the impact of resistance to third/fourth/fifth-generation cephalosporins, resistance to quinolones, and/or multidrug resistance on mortality, treatment failure, length of hospital stay and/or healthcare costs were included. Two researchers independently performed screening, data extraction, and risk of bias assessment. When possible, random effect meta-analyses followed by assessment of the confidence in the cumulative evidence were performed for mortality and length of hospital stay outcomes, and narrative syntheses were performed for treatment failure and healthcare costs.
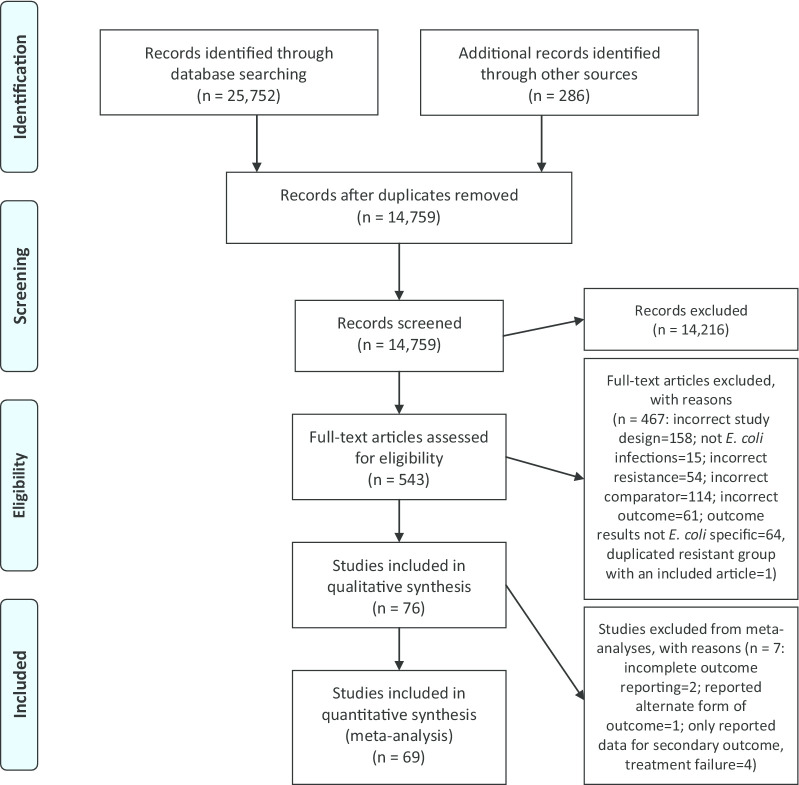
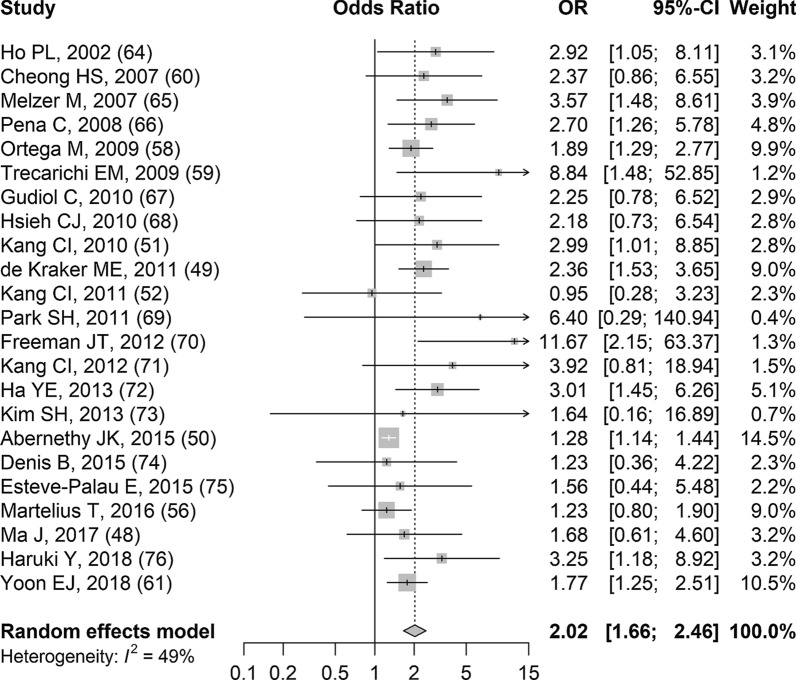
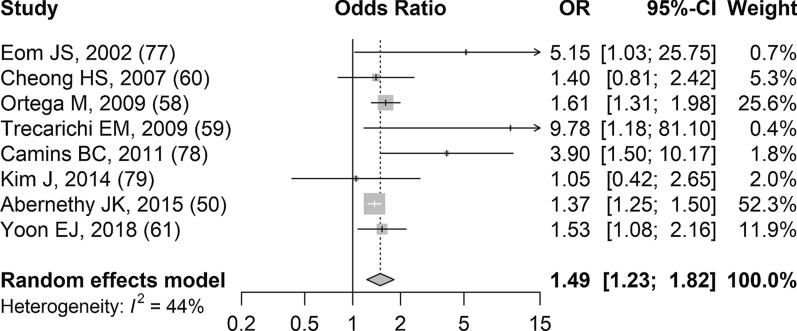
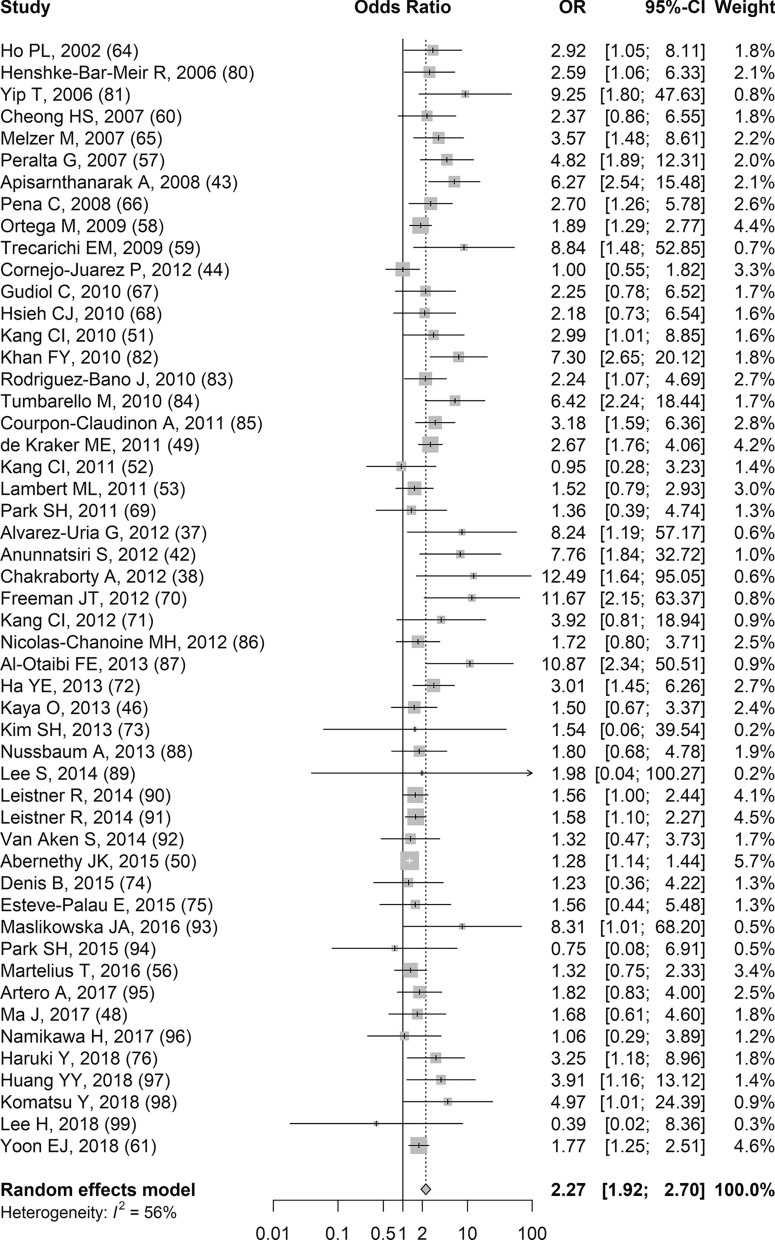
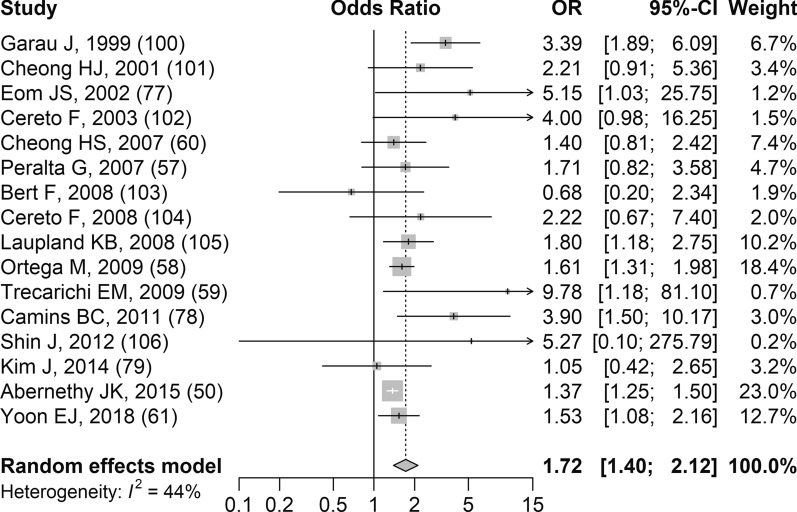
Literature searches identified 14,759 de-duplicated records and 76 articles were included. Based on 30-day and all-cause mortality meta-analyses, regardless of the type of resistance, there was a significant increase in the odds of dying with resistant E. coli infections compared to susceptible infections. A summary mean difference was not presented for total length of hospital stay meta-analyses due to substantial to considerable heterogeneity. Since small numbers of studies contributed to meta-analyses for bacterium-attributable mortality and post-infection length of hospital stay, the summary results should be considered with caution. Studies contributing results for treatment failure and healthcare costs had considerable variability in definitions and reporting.
Overall, resistant E. coli infections were associated with significant 30-day and all-cause mortality burden. More research and/or improved reporting are necessary to facilitate quantitative syntheses of bacterium-attributable mortality, length of hospital stay, and hospital costs. Protocol Registration PROSPERO CRD42018111197.
评估抗菌药物耐药大肠杆菌感染的疾病负担有助于了解问题的严重程度和潜在影响,并与其他疾病进行比较,从而为研究、监测和资金提供优先排序。本研究采用系统评价和荟萃分析方法,旨在评估与敏感大肠杆菌感染相比,患有抗菌药物耐药大肠杆菌感染的人类在健康或卫生保健系统负担方面是否会出现增加。
在四个主要数据库和七个灰色文献数据库中进行了全面的文献检索。纳入了评估第三代/第四代/第五代头孢菌素耐药、喹诺酮耐药和/或多药耐药对死亡率、治疗失败、住院时间和/或医疗保健成本影响的人类大肠杆菌感染的分析性观察研究。两名研究人员独立进行了筛选、数据提取和偏倚风险评估。在可能的情况下,对死亡率和住院时间结局进行了随机效应荟萃分析,然后评估了累积证据的可信度,并对治疗失败和医疗保健成本进行了叙述性综合分析。
文献检索共识别出 14759 条去重记录,纳入了 76 篇文章。基于 30 天和全因死亡率荟萃分析,无论耐药类型如何,与敏感感染相比,耐药大肠杆菌感染患者死亡的几率显著增加。由于汇总的总住院时间存在大量的异质性,因此未呈现荟萃分析的汇总平均差异。由于对细菌归因死亡率和感染后住院时间进行荟萃分析的研究数量较少,因此汇总结果应谨慎考虑。对治疗失败和医疗保健成本进行研究的结果在定义和报告方面存在较大差异。
总的来说,耐药大肠杆菌感染与 30 天和全因死亡率负担显著相关。需要进一步研究和/或改进报告,以促进对细菌归因死亡率、住院时间和住院费用的定量综合分析。注册协议 PROSPERO CRD42018111197。