Cicely Saunders Institute of Palliative Care, Policy and Rehabilitation, King's College London, London, UK
King's Global Health Institute, King's College London, London, UK.
BMJ Glob Health. 2020 Dec;5(12). doi: 10.1136/bmjgh-2020-003330.
Person-centred care has become internationally recognised as a critical attribute of high-quality healthcare. However, the concept has been criticised for being poorly theorised and operationalised. Serious illness is especially aligned with the need for person-centredness, usually necessitating involvement of significant others, management of clinical uncertainty, high-quality communication and joint decision-making to deliver care concordant with patient preferences. This review aimed to identify and appraise the empirical evidence underpinning conceptualisations of 'person-centredness' for serious illness.
Search strategy conducted in May 2020. Databases: CINAHL, Embase, PubMed, Ovid Global Health, MEDLINE and PsycINFO. Free text search terms related to (1) person-centredness, (2) serious illness and (3) concept/practice. Tabulation, textual description and narrative synthesis were performed, and quality appraisal conducted using QualSyst tools. Santana 's person-centred care model (2018) was used to structure analysis.
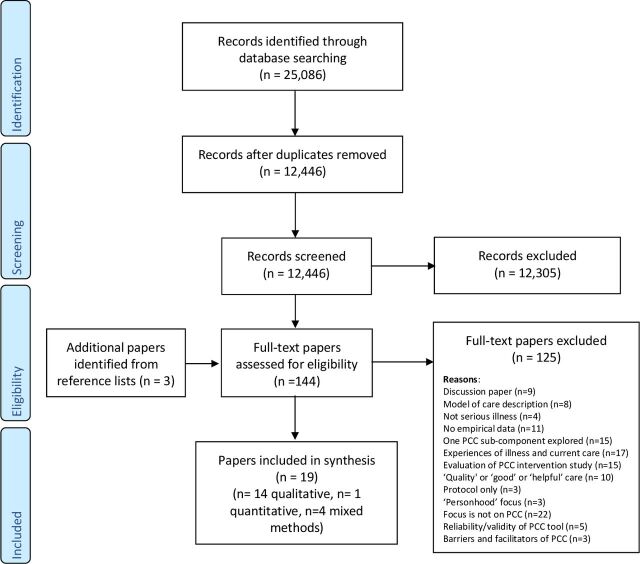
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow data: n=12,446 studies screened by title/abstract, n=144 full articles assessed for eligibility, n=18 studies retained. All studies (n=18) are from high-income countries, and are largely of high quality (median score 0.82). The findings suggest that person-centred care encompasses the patient and family being respected, given complete information, involved in decision-making and supported in their physical, psychological, social and existential needs. The studies highlight the importance of involving and supporting family/friends, promoting continuation of normality and self-identity, and structuring service organisation to enable care continuity.
Person-centred healthcare must value the social network of patients, promote quality of life and reform structurally to improve patients' experience interacting with the healthcare system. Staff must be supported to flexibly adapt skills, communication, routines or environments for individual patients. There remains a need for primary data investigating the meaning and practice of PCC in a greater diversity of diagnostic groups and settings, and a need to ground potential components of PCC within broader universal values and ethical theory.
以患者为中心的护理已在国际上被公认为高质量医疗保健的关键属性。然而,该概念在理论和操作上都受到了批评。严重疾病尤其需要以患者为中心,通常需要涉及重要的他人,管理临床不确定性,进行高质量的沟通和共同决策,以提供符合患者偏好的护理。本综述旨在确定和评估严重疾病患者中心概念的实证证据。
2020 年 5 月进行了搜索策略。数据库:CINAHL、Embase、PubMed、Ovid Global Health、MEDLINE 和 PsycINFO。使用与(1)以患者为中心、(2)严重疾病和(3)概念/实践相关的自由文本搜索词进行搜索。进行制表、文字描述和叙述性综合,并使用 QualSyst 工具进行质量评估。使用 Santana 的以患者为中心的护理模型(2018 年)对分析进行结构。
PRISMA(系统评价和荟萃分析的首选报告项目)流程图数据:通过标题/摘要筛选的 n=12446 项研究,n=144 篇全文评估合格,n=18 项研究保留。所有研究(n=18)均来自高收入国家,且质量大多较高(中位数评分为 0.82)。研究结果表明,以患者为中心的护理包括尊重患者和家属,提供完整的信息,让他们参与决策,并支持他们的身体、心理、社会和存在需求。这些研究强调了让家人/朋友参与和支持、促进正常生活和自我认同的延续以及构建服务组织以实现护理连续性的重要性。
以患者为中心的医疗保健必须重视患者的社交网络,提高生活质量,并进行结构性改革,以改善患者与医疗保健系统的互动体验。必须支持工作人员灵活调整技能、沟通、常规或环境,以满足个别患者的需求。需要对以患者为中心的护理的意义和实践进行更多的实证研究,以更大的多样性诊断群体和环境为背景,并需要将以患者为中心的护理的潜在组成部分建立在更广泛的普遍价值观和伦理理论之上。