Coomans Marijke B, Taphoorn Martin J B, Aaronson Neil K, Baumert Brigitta G, van den Bent Martin, Bottomley Andrew, Brandes Alba A, Chinot Olivier, Coens Corneel, Gorlia Thierry, Herrlinger Ulrich, Keime-Guibert Florence, Malmström Annika, Martinelli Francesca, Stupp Roger, Talacchi Andrea, Weller Michael, Wick Wolfgang, Reijneveld Jaap C, Dirven Linda
Department of Neurology, Leiden University Medical Center, Leiden, the Netherlands.
Department of Neurology, Haaglanden Medical Center, Den Haag, the Netherlands.
Neurooncol Pract. 2020 Jun 7;7(6):668-675. doi: 10.1093/nop/npaa033. eCollection 2020 Dec.
Different analytical methods may lead to different conclusions about the impact of treatment on health-related quality of life (HRQoL). This study aimed to examine 3 different methods to evaluate change in HRQoL and to study whether these methods result in different conclusions.
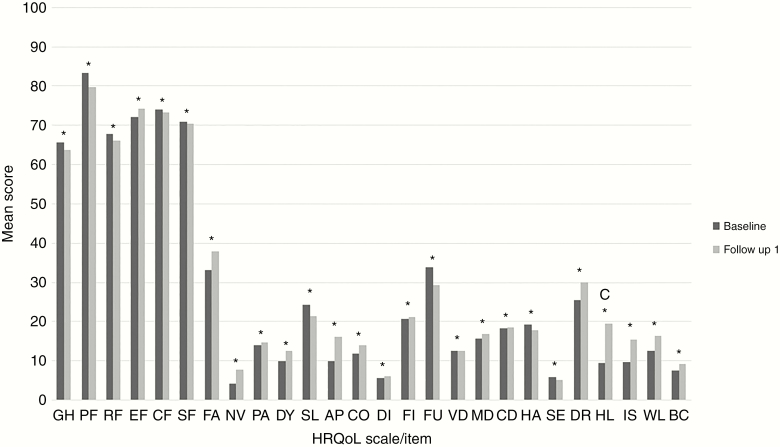
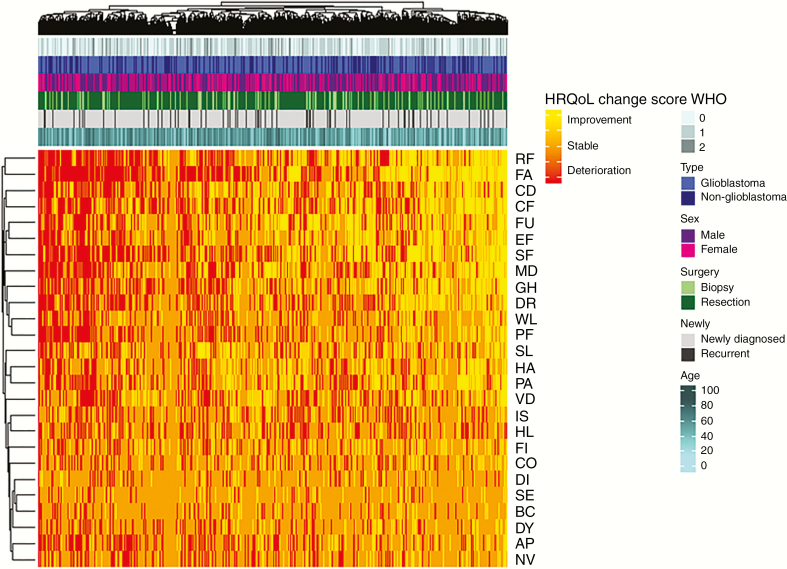
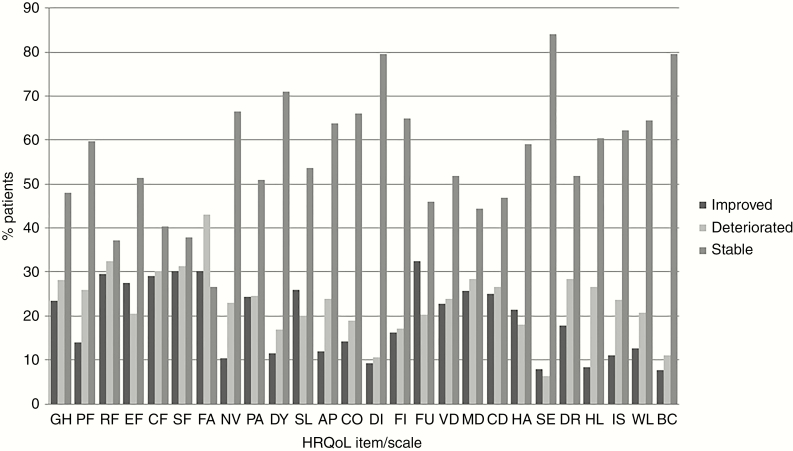
HRQoL data from 15 randomized clinical trials were combined (CODAGLIO project). Change in HRQoL scores, measured with the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 and BN20 questionnaires, was analyzed in 3 ways: (1) at the group level, comparing mean changes in scale/item scores between treatment arms, (2) at the patient level per scale/item, calculating the percentage of patients that deteriorated, improved, or remained stable per scale/item, and (3) at the individual patient level, combining all scales/items.
Baseline and first follow-up HRQoL data were available for 3727 patients. At the group scale/item level, only the item "hair loss" showed a significant and clinically relevant change (ie, ≥10 points) over time, whereas change scores on the other scales/items were statistically significant only (all < .001; range in change score, 0.1-6.2). Although a large proportion of patients had stable HRQoL over time (range, 27%-84%) on the patient level per scale/item, many patients deteriorated (range, 6%-43%) or improved (range, 8%-32%) on a specific scale/item. At the individual patient level, the majority of patients (86%) showed both deterioration and improvement, whereas only 1% remained stable on all scales.
Different analytical methods of changes in HRQoL result in distinct conclusions of treatment effects, all of which may be relevant for informing clinical decision making.
不同的分析方法可能会对治疗对健康相关生活质量(HRQoL)的影响得出不同结论。本研究旨在检验三种评估HRQoL变化的不同方法,并研究这些方法是否会得出不同结论。
合并了来自15项随机临床试验的HRQoL数据(CODAGLIO项目)。使用欧洲癌症研究与治疗组织生活质量问卷核心30和BN20问卷测量的HRQoL得分变化,通过三种方式进行分析:(1)在组水平上,比较各治疗组间量表/条目的平均得分变化;(2)在每个量表/条目的患者水平上,计算每个量表/条目恶化、改善或保持稳定的患者百分比;(3)在个体患者水平上,合并所有量表/条目。
共有3727例患者有基线和首次随访的HRQoL数据。在组量表/条目水平上,只有“脱发”条目随时间显示出显著且具有临床意义的变化(即≥10分),而其他量表/条目的变化得分仅具有统计学意义(均<0.001;变化得分范围为0.1 - 6.2)。尽管在每个量表/条目的患者水平上,很大一部分患者的HRQoL随时间保持稳定(范围为27% - 84%),但许多患者在特定量表/条目上出现了恶化(范围为6% - 43%)或改善(范围为8% - 32%)。在个体患者水平上,大多数患者(86%)既有恶化又有改善,而只有1%的患者在所有量表上都保持稳定。
HRQoL变化的不同分析方法会得出关于治疗效果的不同结论,所有这些结论可能都与临床决策相关。