Upadhyay Ushma D, Schroeder Rosalyn, Roberts Sarah C M
Advancing New Standards in Reproductive Health (ANSIRH), Dept. of Obstetrics, Gynecology & Reproductive Sciences, University of California, San Francisco, 1330 Broadway, Suite 1100, Oakland, CA 94612.
Contracept X. 2020 Nov 21;2:100049. doi: 10.1016/j.conx.2020.100049. eCollection 2020.
Access to abortion care in the United States (US) is restricted by numerous logistical and financial barriers, which have been further intensified by the COVID-19 pandemic. We sought to understand the ways in which COVID-19 prompted changes in clinical practices in abortion care among independent abortion clinics.
We surveyed independent US abortion clinics and documented changes in practice regarding the provision of abortion since March 1, 2020.
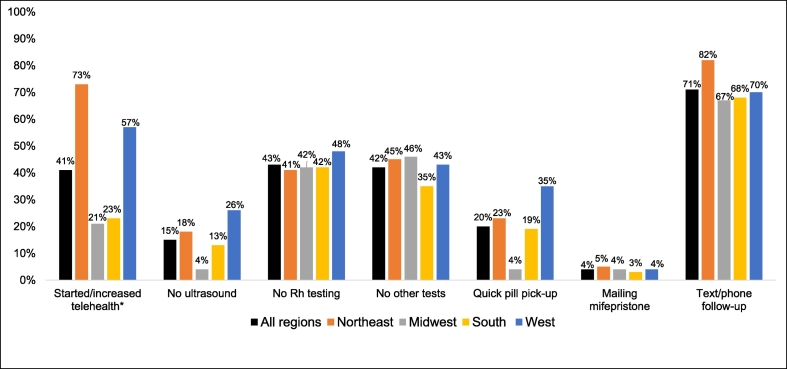
Among about 153 independent clinics invited, 100 clinics contributed relevant data and were included in the analytic sample. A total of 87% reported changes in protocols in response to the COVID-19 pandemic. Reported changes included moving to telehealth (phone or video) for follow-up (71%), starting or increasing telehealth for patient consultations and screening (41%), reducing Rh testing (43%) and other tests (42%), and omitting the preabortion ultrasound (15%). A total of 20% reported allowing quick pickup of medication abortion pills, and 4% began mailing medications directly to patients after a telehealth consultation. Clinical practice changes were reported throughout all regions of the US, but facilities in the Northeast (73%) were more likely to report starting or increasing telehealth than facilities in the South (23%, p < .001).
The COVID-19 pandemic accelerated use of telehealth among independent abortion clinics, but many clinics, particularly those in the South, have been unable to make these changes. Other practices such as reducing preabortion ultrasounds were less common in all regions despite clinical guidelines and evidence supporting such changes in practice and positive benefits for public health and patient-centered care.
The COVID-19 pandemic has created a window of opportunity to remove barriers to abortion, including expanding telehealth and reducing preabortion tests. Clinics can strive for a culture shift towards simplifying the provision of medication abortion and routinely avoiding preabortion tests and in-person visits. Such changes in practice could have positive benefits for public health and patient-centered care.
在美国,获得堕胎护理受到众多后勤和经济障碍的限制,而新冠疫情进一步加剧了这些障碍。我们试图了解新冠疫情促使独立堕胎诊所的堕胎护理临床实践发生变化的方式。
我们对美国独立堕胎诊所进行了调查,并记录了自2020年3月1日以来堕胎服务提供方面的实践变化。
在约153家受邀的独立诊所中,100家诊所提供了相关数据并被纳入分析样本。共有87%的诊所报告称,为应对新冠疫情,其协议发生了变化。报告的变化包括转向远程医疗(电话或视频)进行随访(71%)、开始或增加远程医疗进行患者咨询和筛查(41%)、减少Rh检测(43%)和其他检测(42%),以及省略堕胎前超声检查(15%)。共有20%的诊所报告允许快速领取药物流产药片,4%的诊所开始在远程医疗咨询后直接将药物邮寄给患者。美国所有地区都报告了临床实践的变化,但东北部的机构(73%)比南部的机构(23%,p<0.001)更有可能报告开始或增加远程医疗服务。
新冠疫情加速了独立堕胎诊所对远程医疗的使用,但许多诊所,尤其是南部的诊所,无法做出这些改变。尽管临床指南和证据支持这种实践变化以及对公共卫生和以患者为中心的护理有积极益处,但减少堕胎前超声检查等其他实践在所有地区都不太常见。
新冠疫情创造了一个消除堕胎障碍的机会之窗,包括扩大远程医疗和减少堕胎前检测。诊所可以努力实现文化转变,简化药物流产的提供流程,常规性地避免堕胎前检测和面对面就诊。这种实践变化可能对公共卫生和以患者为中心的护理产生积极益处。