National Kunming High-Level Biosafety Primate Research Center, Institute of Medical Biology, Chinese Academy of Medical Sciences and Peking Union Medical College, Yunnan, China.
National Kunming High-Level Biosafety Primate Research Center, Institute of Medical Biology, Chinese Academy of Medical Sciences and Peking Union Medical College, Yunnan, China; State Key Laboratory of Medical Molecular Biology, Department of Molecular Biology and Biochemistry, Institute of Basic Medical Sciences, Medical Primate Research Center, Neuroscience Center, Chinese Academy of Medical Sciences, School of Basic Medicine Peking Union Medical College, Beijing, China.
Gastroenterology. 2021 Apr;160(5):1647-1661. doi: 10.1053/j.gastro.2020.12.001. Epub 2020 Dec 9.
BACKGROUND & AIMS: Gastrointestinal (GI) manifestations have been increasingly reported in patients with coronavirus disease 2019 (COVID-19). However, the roles of the GI tract in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are not fully understood. We investigated how the GI tract is involved in SARS-CoV-2 infection to elucidate the pathogenesis of COVID-19.
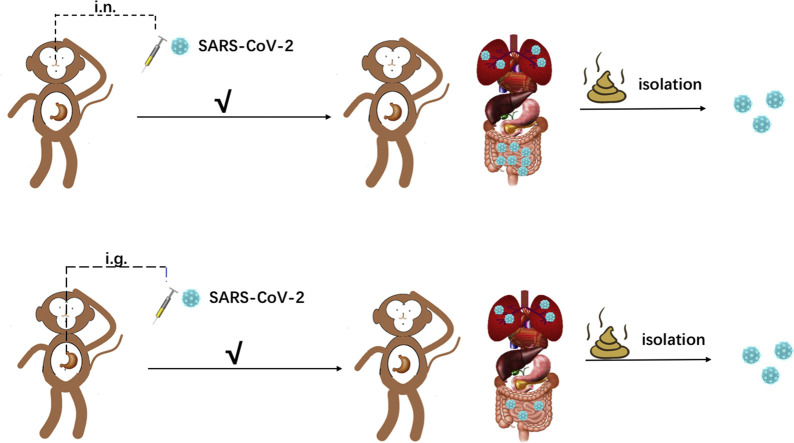
Our previously established nonhuman primate (NHP) model of COVID-19 was modified in this study to test our hypothesis. Rhesus monkeys were infected with an intragastric or intranasal challenge with SARS-CoV-2. Clinical signs were recorded after infection. Viral genomic RNA was quantified by quantitative reverse transcription polymerase chain reaction. Host responses to SARS-CoV-2 infection were evaluated by examining inflammatory cytokines, macrophages, histopathology, and mucin barrier integrity.
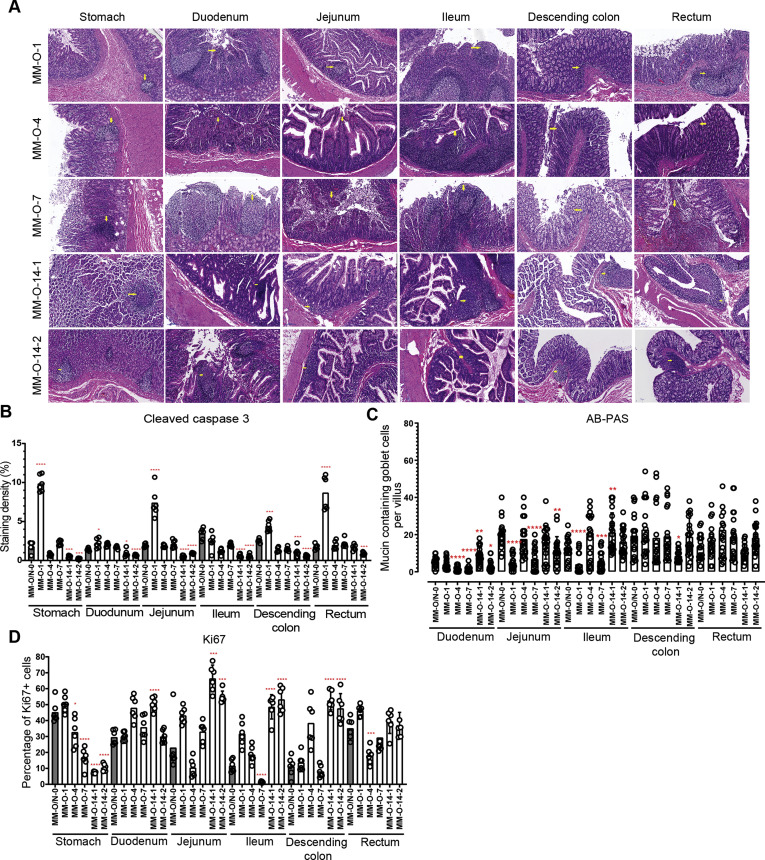
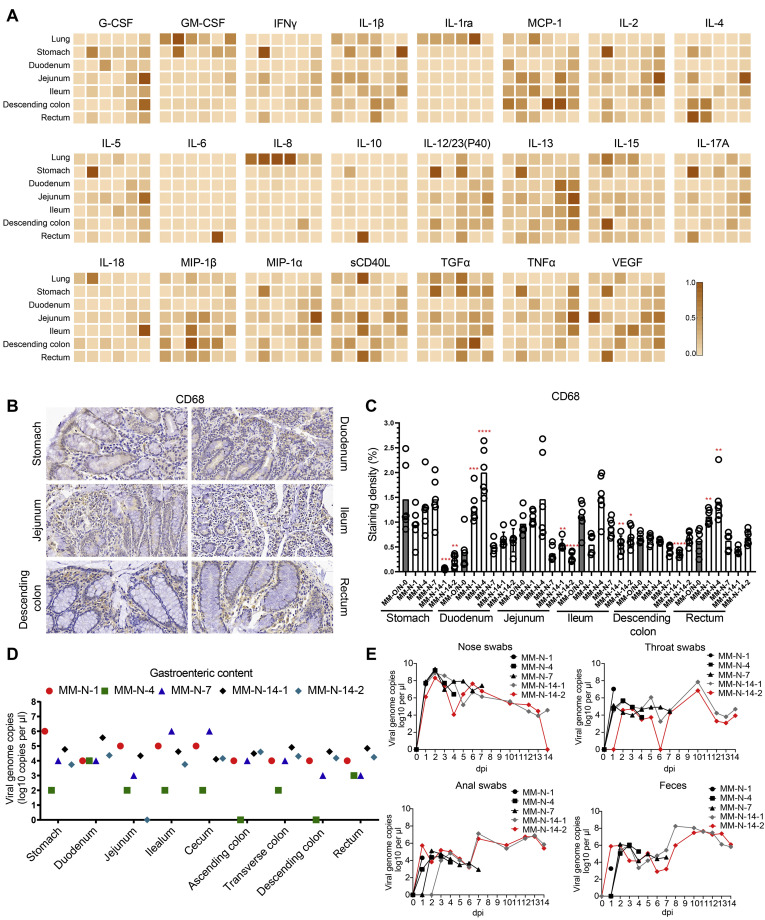
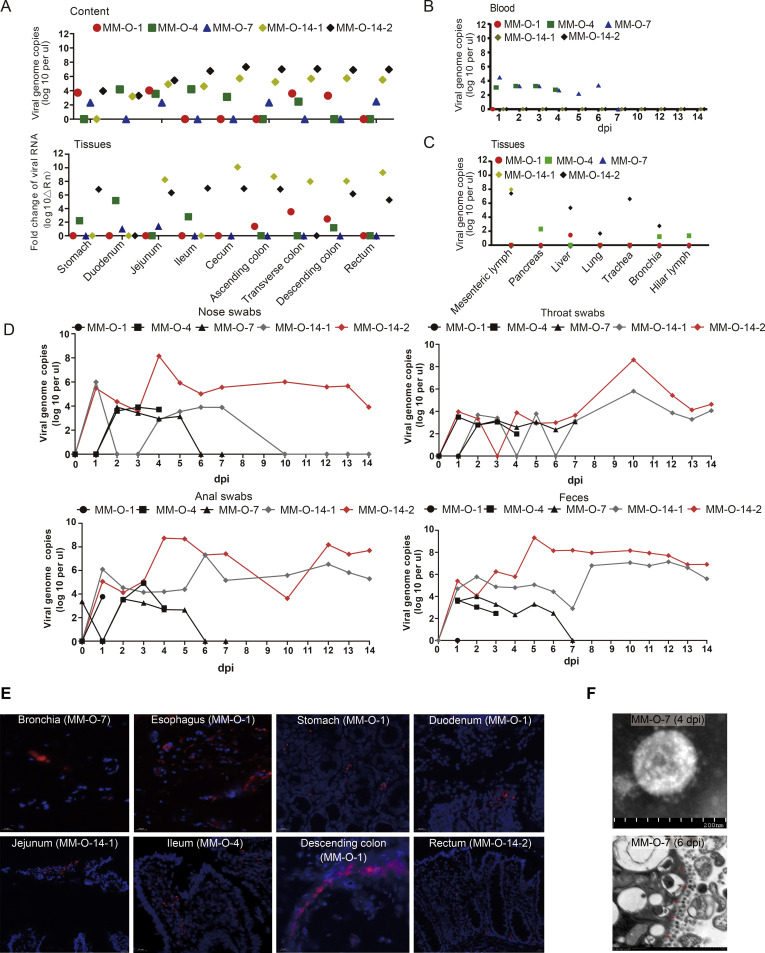
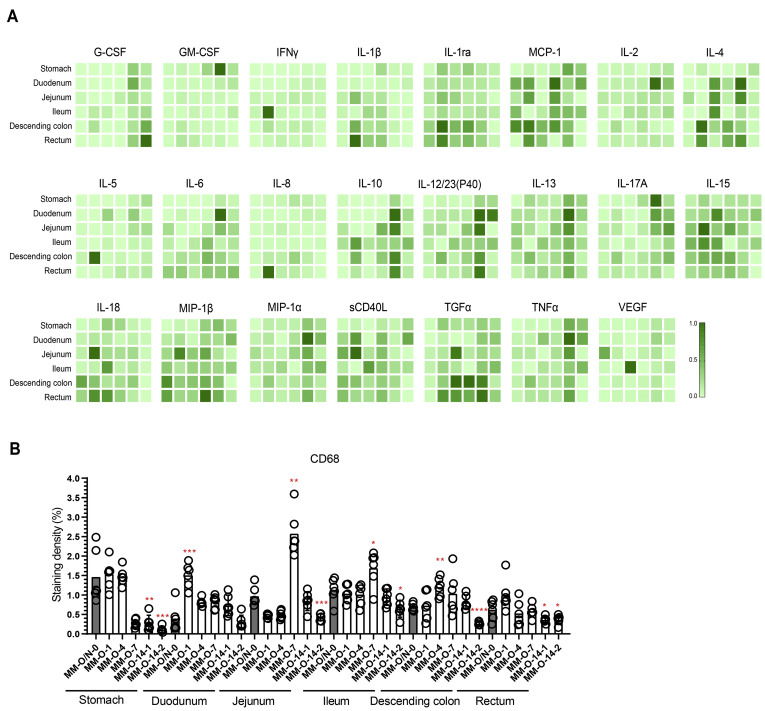
Intranasal inoculation with SARS-CoV-2 led to infections and pathologic changes not only in respiratory tissues but also in digestive tissues. Expectedly, intragastric inoculation with SARS-CoV-2 resulted in the productive infection of digestive tissues and inflammation in both the lung and digestive tissues. Inflammatory cytokines were induced by both types of inoculation with SARS-CoV-2, consistent with the increased expression of CD68. Immunohistochemistry and Alcian blue/periodic acid-Schiff staining showed decreased Ki67, increased cleaved caspase 3, and decreased numbers of mucin-containing goblet cells, suggesting that the inflammation induced by these 2 types of inoculation with SARS-CoV-2 impaired the GI barrier and caused severe infections.
Both intranasal and intragastric inoculation with SARS-CoV-2 caused pneumonia and GI dysfunction in our rhesus monkey model. Inflammatory cytokines are possible connections for the pathogenesis of SARS-CoV-2 between the respiratory and digestive systems.
越来越多的研究报道了 2019 年冠状病毒病(COVID-19)患者存在胃肠道(GI)表现。然而,GI 道在严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染中的作用尚未完全阐明。我们研究了 SARS-CoV-2 感染中 GI 道的作用,以阐明 COVID-19 的发病机制。
本研究对我们之前建立的 COVID-19 非人类灵长类动物(NHP)模型进行了修改,以验证我们的假设。恒河猴通过经口或经鼻感染 SARS-CoV-2。感染后记录临床症状。通过定量逆转录聚合酶链反应(qRT-PCR)定量病毒基因组 RNA。通过检测炎症细胞因子、巨噬细胞、组织病理学和粘蛋白屏障完整性,评估宿主对 SARS-CoV-2 感染的反应。
经鼻接种 SARS-CoV-2 不仅导致呼吸道组织感染和病理改变,还导致消化道组织感染和病理改变。预期的是,经口接种 SARS-CoV-2 导致消化道组织的感染和肺部及消化道组织的炎症。两种接种方式均诱导了炎症细胞因子的产生,与 CD68 表达增加一致。免疫组化和阿尔辛蓝/过碘酸希夫染色显示 Ki67 减少、cleaved caspase 3 增加和含粘蛋白的杯状细胞数量减少,表明这两种接种方式诱导的炎症损害了 GI 屏障并导致严重感染。
本研究的恒河猴模型中,经鼻和经口接种 SARS-CoV-2 均导致肺炎和 GI 功能障碍。炎症细胞因子可能是 SARS-CoV-2 引起呼吸系统和消化系统发病机制的联系。