MOE-Shanghai Key Laboratory of Children's Environmental Health, Xin Hua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Department of Epidemiology, University Medical Center Groningen, Groningen, The Netherlands.
BMC Infect Dis. 2020 Dec 17;20(1):959. doi: 10.1186/s12879-020-05688-y.
Previous published prognostic models for COVID-19 patients have been suggested to be prone to bias due to unrepresentativeness of patient population, lack of external validation, inappropriate statistical analyses, or poor reporting. A high-quality and easy-to-use prognostic model to predict in-hospital mortality for COVID-19 patients could support physicians to make better clinical decisions.
Fine-Gray models were used to derive a prognostic model to predict in-hospital mortality (treating discharged alive from hospital as the competing event) in COVID-19 patients using two retrospective cohorts (n = 1008) in Wuhan, China from January 1 to February 10, 2020. The proposed model was internally evaluated by bootstrap approach and externally evaluated in an external cohort (n = 1031).
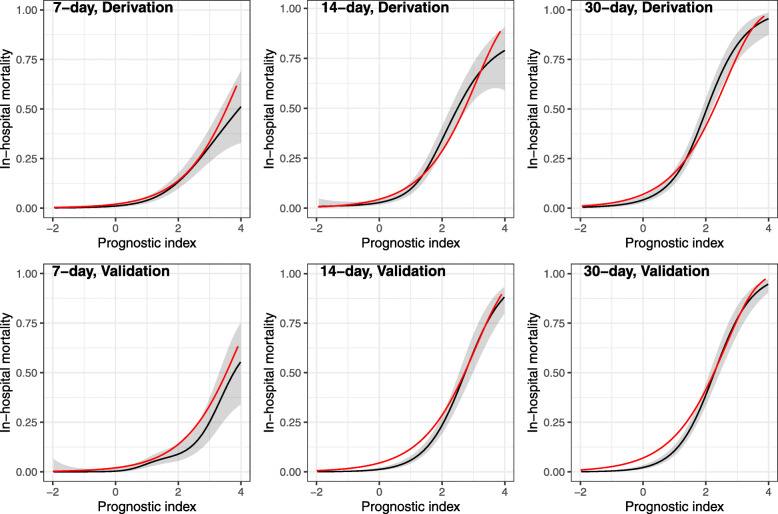
The derivation cohort was a case-mix of mild-to-severe hospitalized COVID-19 patients (43.6% females, median age 55). The final model (PLANS), including five predictor variables of platelet count, lymphocyte count, age, neutrophil count, and sex, had an excellent predictive performance (optimism-adjusted C-index: 0.85, 95% CI: 0.83 to 0.87; averaged calibration slope: 0.95, 95% CI: 0.82 to 1.08). Internal validation showed little overfitting. External validation using an independent cohort (47.8% female, median age 63) demonstrated excellent predictive performance (C-index: 0.87, 95% CI: 0.85 to 0.89; calibration slope: 1.02, 95% CI: 0.92 to 1.12). The averaged predicted cumulative incidence curves were close to the observed cumulative incidence curves in patients with different risk profiles.
The PLANS model based on five routinely collected predictors would assist clinicians in better triaging patients and allocating healthcare resources to reduce COVID-19 fatality.
先前发表的 COVID-19 患者预后模型由于患者人群代表性不足、缺乏外部验证、不适当的统计分析或报告不当而存在偏差。一个高质量且易于使用的预测 COVID-19 患者住院死亡率的预后模型可以帮助医生做出更好的临床决策。
使用 Fine-Gray 模型从 2020 年 1 月 1 日至 2 月 10 日在中国武汉的两个回顾性队列(n=1008)中得出一个预测住院死亡率(将出院存活视为竞争事件)的预后模型。该模型通过自举法进行内部评估,并在外部队列(n=1031)中进行外部评估。
该队列包括轻至重度住院 COVID-19 患者(43.6%为女性,中位年龄为 55 岁)。最终模型(PLANS)包括血小板计数、淋巴细胞计数、年龄、中性粒细胞计数和性别五个预测变量,具有出色的预测性能(校正后的乐观 C 指数:0.85,95%置信区间:0.83 至 0.87;平均校准斜率:0.95,95%置信区间:0.82 至 1.08)。内部验证显示拟合度良好。使用独立队列(47.8%为女性,中位年龄为 63 岁)进行外部验证表明,该模型具有出色的预测性能(C 指数:0.87,95%置信区间:0.85 至 0.89;校准斜率:1.02,95%置信区间:0.92 至 1.12)。对于不同风险特征的患者,平均预测累积发病率曲线与观察到的累积发病率曲线接近。
基于五个常规收集的预测因子的 PLANS 模型将帮助临床医生更好地对患者进行分诊,并分配医疗资源以降低 COVID-19 的死亡率。