Halabchi Farzin, Hassabi Mohammad
Department of Sports and Exercise Medicine, Tehran University of Medical Sciences, Tehran 14167-53955, Iran.
Department of Sports and Exercise Medicine, Shahid Beheshti University of Medical Sciences, Tehran 19979-64151, Iran.
World J Orthop. 2020 Dec 18;11(12):534-558. doi: 10.5312/wjo.v11.i12.534.
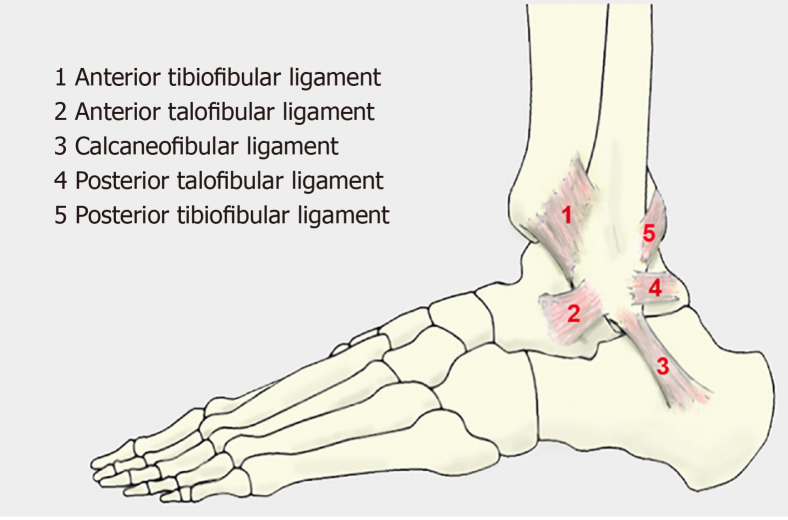
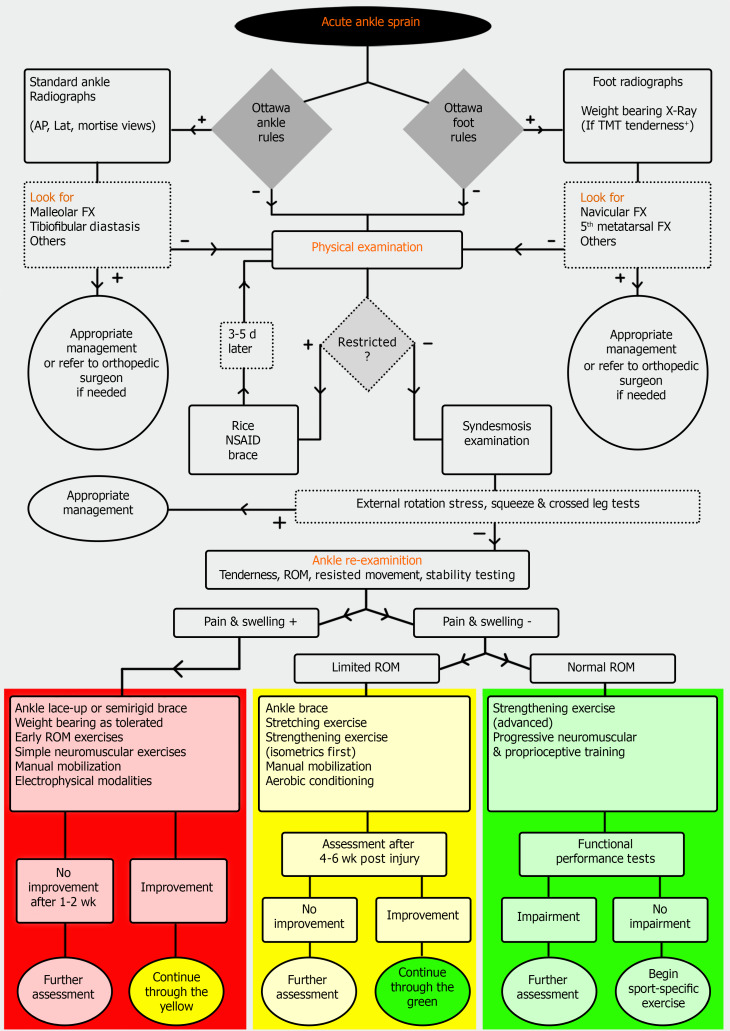
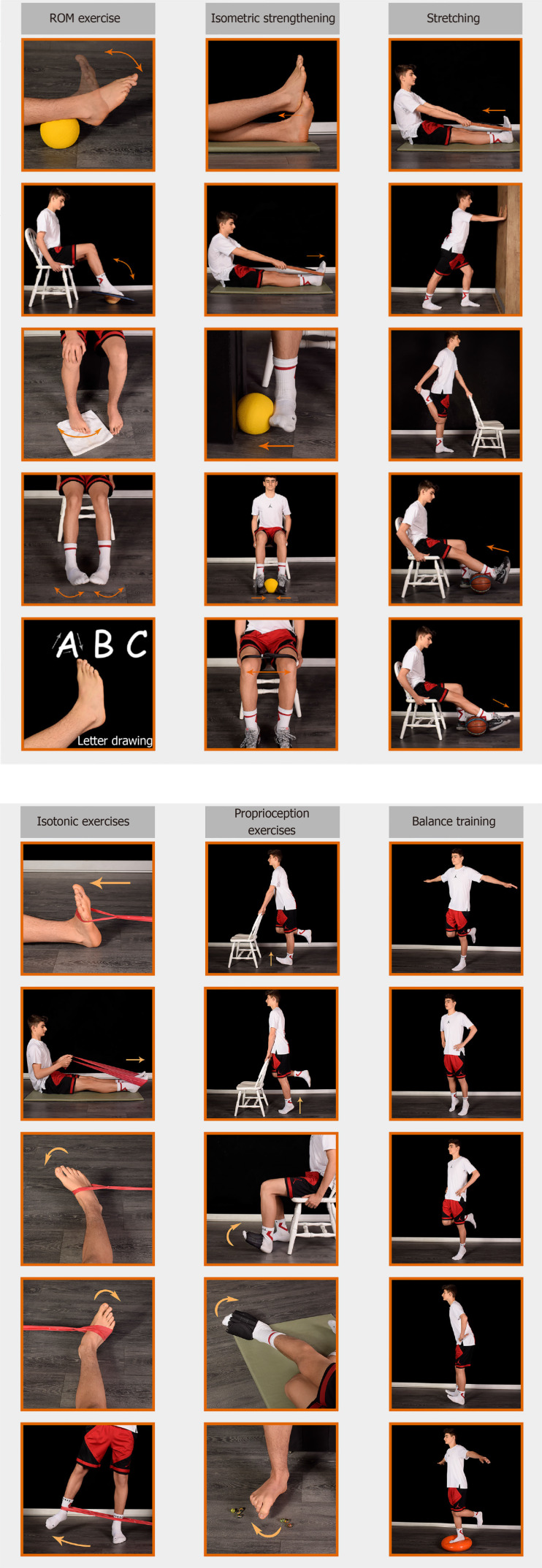
Acute ankle sprain is the most common lower limb injury in athletes and accounts for 16%-40% of all sports-related injuries. It is especially common in basketball, American football, and soccer. The majority of sprains affect the lateral ligaments, particularly the anterior talofibular ligament. Despite its high prevalence, a high proportion of patients experience persistent residual symptoms and injury recurrence. A detailed history and proper physical examination are diagnostic cornerstones. Imaging is not indicated for the majority of ankle sprain cases and should be requested according to the Ottawa ankle rules. Several interventions have been recommended in the management of acute ankle sprains including rest, ice, compression, and elevation, analgesic and anti-inflammatory medications, bracing and immobilization, early weight-bearing and walking aids, foot orthoses, manual therapy, exercise therapy, electrophysical modalities and surgery (only in selected refractory cases). Among these interventions, exercise and bracing have been recommended with a higher level of evidence and should be incorporated in the rehabilitation process. An exercise program should be comprehensive and progressive including the range of motion, stretching, strengthening, neuromuscular, proprioceptive, and sport-specific exercises. Decision-making regarding return to the sport in athletes may be challenging and a sports physician should determine this based on the self-reported variables, manual tests for stability, and functional performance testing. There are some common myths and mistakes in the management of ankle sprains, which all clinicians should be aware of and avoid. These include excessive imaging, unwarranted non-weight-bearing, unjustified immobilization, delay in functional movements, and inadequate rehabilitation. The application of an evidence-based algorithmic approach considering the individual characteristics is helpful and should be recommended.
急性踝关节扭伤是运动员中最常见的下肢损伤,占所有运动相关损伤的16%-40%。在篮球、美式足球和足球运动中尤为常见。大多数扭伤影响外侧韧带,尤其是距腓前韧带。尽管其发病率很高,但仍有很大比例的患者会出现持续的残留症状和损伤复发。详细的病史和适当的体格检查是诊断的基石。大多数踝关节扭伤病例无需影像学检查,应根据渥太华踝关节规则进行检查。在急性踝关节扭伤的治疗中,推荐了几种干预措施,包括休息、冰敷、加压包扎和抬高患肢、止痛和抗炎药物、支具固定、早期负重和助行器、足部矫形器、手法治疗、运动疗法、电物理治疗和手术(仅适用于某些难治性病例)。在这些干预措施中,运动和支具固定的推荐证据级别较高,应纳入康复过程。运动计划应全面且循序渐进,包括关节活动范围、拉伸、增强肌力、神经肌肉、本体感觉和特定运动的练习。对于运动员何时恢复运动的决策可能具有挑战性,运动医生应根据自我报告的变量、稳定性的手法测试和功能表现测试来做出决定。在踝关节扭伤的治疗中存在一些常见的误区和错误,所有临床医生都应了解并避免。这些包括过度的影像学检查、不必要的不负重、不合理的固定、功能活动延迟和康复不足。应用考虑个体特征的循证算法方法是有帮助的,应该予以推荐。