Department of Environmental Medicine and Behavioral Science, Kindai University Faculty of Medicine, Osakasayama 589-8511, Japan.
Environ Int. 2021 Feb;147:106338. doi: 10.1016/j.envint.2020.106338. Epub 2020 Dec 23.
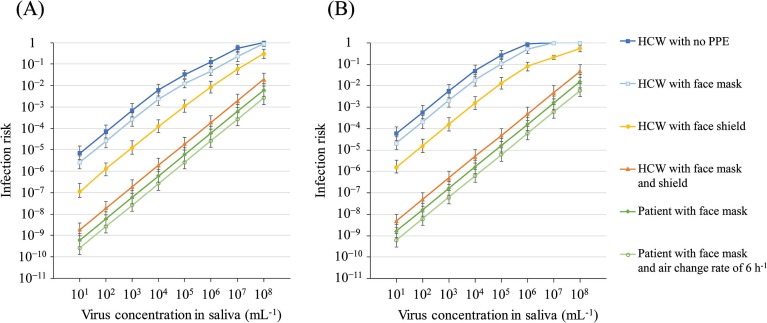
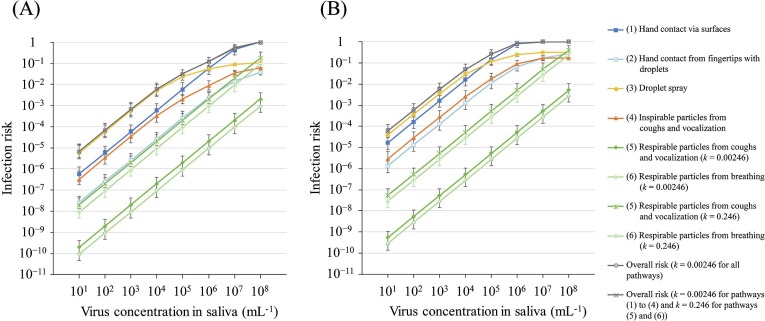
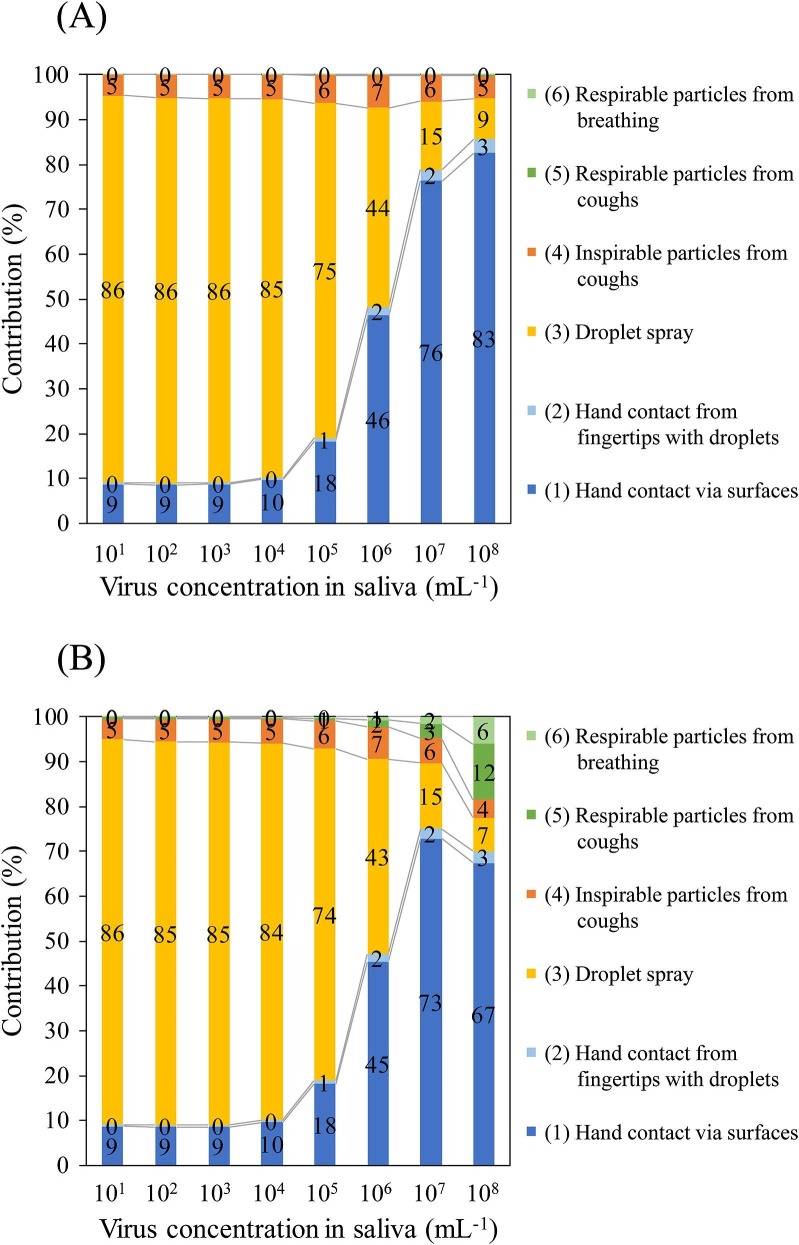
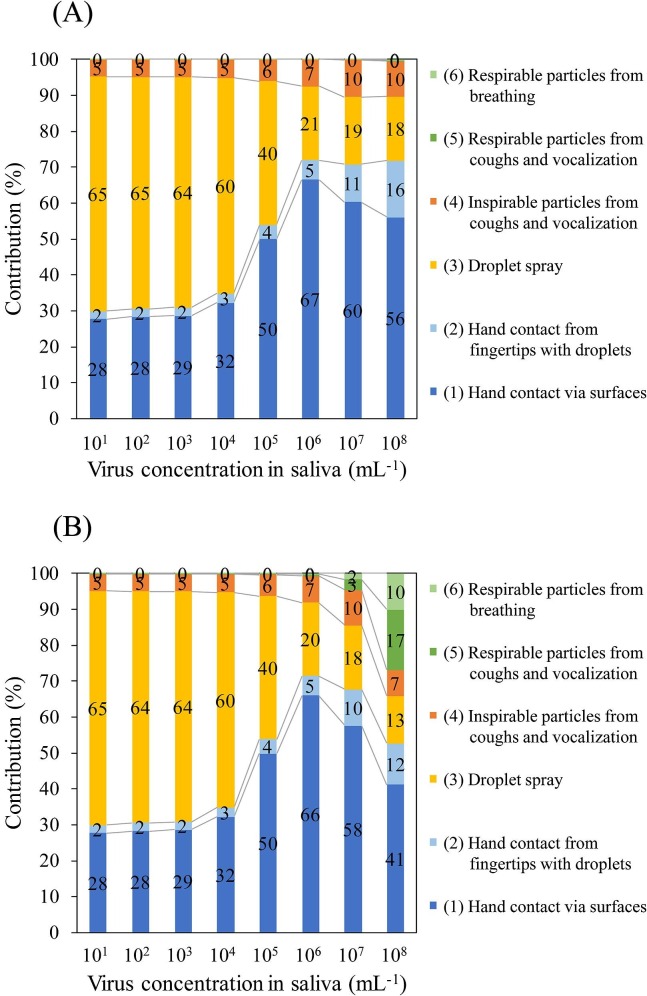
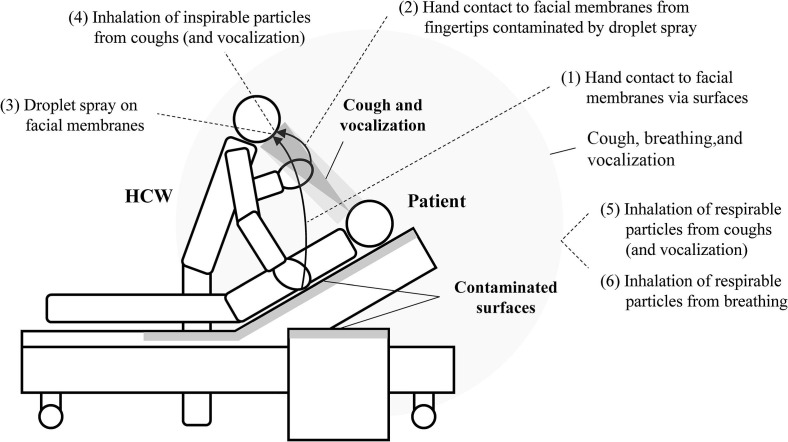
We assessed the risk of COVID-19 infection in a healthcare worker (HCW) from multiple pathways of exposure to SARS-CoV-2 in a health-care setting of short distance of 0.6 m between the HCW and a patient while caring, and evaluated the effectiveness of a face mask and a face shield using a model that combined previous infection-risk models. The multiple pathways of exposure included hand contact via contaminated surfaces and an HCW's fingers with droplets, droplet spray, and inhalation of inspirable and respirable particles. We assumed a scenario of medium contact time (MCT) and long contact time (LCT) over 1 day of care by an HCW. SARS-CoV-2 in the particles emitted by coughing, breathing, and vocalization (only in the LCT scenario) by the patient were considered. The contribution of the risk of infection of an HCW by SARS-CoV-2 from each pathway to the sum of the risks from all pathways depended on virus concentration in the saliva of the patient. At a virus concentration in the saliva of 10-10 PFU mL concentration in the MCT scenario and 10-10 PFU mL concentration in the LCT scenario, droplet spraying was the major pathway (60%-86%) of infection, followed by hand contact via contaminated surfaces (9%-32%). At a high virus concentration in the saliva (10-10 PFU mL in the MCT scenario and 10-10 PFU mL in the LCT scenario), hand contact via contaminated surfaces was the main contributor (41%-83%) to infection. The contribution of inhalation of inspirable particles was 4%-10% in all assumed cases. The contribution of inhalation of respirable particles increased as the virus concentration in the saliva increased, and reached 5%-27% at the high saliva concentration (10 and 10 PFU mL) in the assumed scenarios using higher dose-response function parameter (0.246) and comparable to other pathways, although these were worst and rare cases. Regarding the effectiveness of nonpharmaceutical interventions, the relative risk (RR) of an overall risk for an HCW with an intervention vs. an HCW without intervention was 0.36-0.37, 0.02-0.03, and <4.0 × 10 for a face mask, a face shield, and a face mask plus shield, respectively, in the likely median virus concentration in the saliva (10-10 PFU mL), suggesting that personal protective equipment decreased the infection risk by 63%->99.9%. In addition, the RR for a face mask worn by the patient, and a face mask worn by the patient plus increase of air change rate from 2 h to 6 h was <1.0 × 10 and <5.0 × 10, respectively in the same virus concentration in the saliva. Therefore, by modeling multiple pathways of exposure, the contribution of the infection risk from each pathway and the effectiveness of nonpharmaceutical interventions for COVID-19 were indicated quantitatively, and the importance of the use of a face mask and shield was confirmed.
我们评估了医护人员(HCW)在医疗环境中接触 SARS-CoV-2 的多种途径的 COVID-19 感染风险,这些接触途径包括 HCW 在护理过程中与患者之间的近距离(0.6 m)、接触受污染表面的手以及 HCW 手指上的飞沫、飞沫喷雾以及可吸入和可呼吸颗粒的吸入。我们假设 HCW 在一天的护理中存在中接触时间(MCT)和长接触时间(LCT)两种情况。考虑了患者咳嗽、呼吸和发声(仅在 LCT 情况下)时颗粒中 SARS-CoV-2 的情况。每个途径中 SARS-CoV-2 感染 HCW 的风险在所有途径风险总和中的贡献取决于患者唾液中的病毒浓度。在 MCT 场景中病毒浓度为 10-10 PFU mL 和 LCT 场景中病毒浓度为 10-10 PFU mL 的情况下,飞沫喷雾是感染的主要途径(60%-86%),其次是接触受污染表面的手(9%-32%)。在高病毒浓度的唾液(MCT 场景中为 10-10 PFU mL 和 LCT 场景中为 10-10 PFU mL)中,接触受污染表面是感染的主要贡献者(41%-83%)。在所有假设情况下,可吸入颗粒的吸入贡献为 4%-10%。随着唾液中病毒浓度的增加,可吸入颗粒的吸入贡献增加,在假设情况下使用更高的剂量反应函数参数(0.246)和与其他途径相当的情况下,最高可达到 5%-27%,尽管这些情况是最坏和罕见的情况。关于非药物干预措施的有效性,干预组和未干预组医护人员的总风险的相对风险(RR)分别为 0.36-0.37、0.02-0.03 和 <4.0×10,对于在可能的唾液中位数病毒浓度(10-10 PFU mL)中使用的口罩、面罩和口罩加面罩,这表明个人防护设备降低了 63%->99.9%的感染风险。此外,在相同病毒浓度的唾液中,患者佩戴口罩和患者佩戴口罩加上空气交换率从 2 小时增加到 6 小时的 RR 分别为 <1.0×10 和 <5.0×10。因此,通过对多种暴露途径进行建模,定量地表明了每种途径的感染风险的贡献和非药物干预措施的有效性,并证实了使用口罩和面罩的重要性。