Callahan Kathryn E, Clark Clancy J, Edwards Angela F, Harwood Timothy N, Williamson Jeff D, Moses Adam W, Willard James J, Cristiano Joseph A, Meadows Kellice, Hurie Justin, High Kevin P, Meredith J Wayne, Pajewski Nicholas M
Section on Gerontology and Geriatric Medicine, Department of Internal Medicine, Wake Forest School of Medicine, Winston-Salem, North Carolina, USA.
Center for Health Care Innovation, Wake Forest School of Medicine, Winston-Salem, North Carolina, USA.
J Am Geriatr Soc. 2021 May;69(5):1357-1362. doi: 10.1111/jgs.17027. Epub 2021 Jan 19.
Frailty is associated with numerous post-operative adverse outcomes in older adults. Current pre-operative frailty screening tools require additional data collection or objective assessments, adding expense and limiting large-scale implementation.
To evaluate the association of an automated measure of frailty integrated within the Electronic Health Record (EHR) with post-operative outcomes for nonemergency surgeries.
Retrospective cohort study.
Academic Medical Center.
Patients 65 years or older that underwent nonemergency surgery with an inpatient stay 24 hours or more between October 8th, 2017 and June 1st, 2019.
Frailty as measured by a 54-item electronic frailty index (eFI).
Inpatient length of stay, requirements for post-acute care, 30-day readmission, and 6-month all-cause mortality.
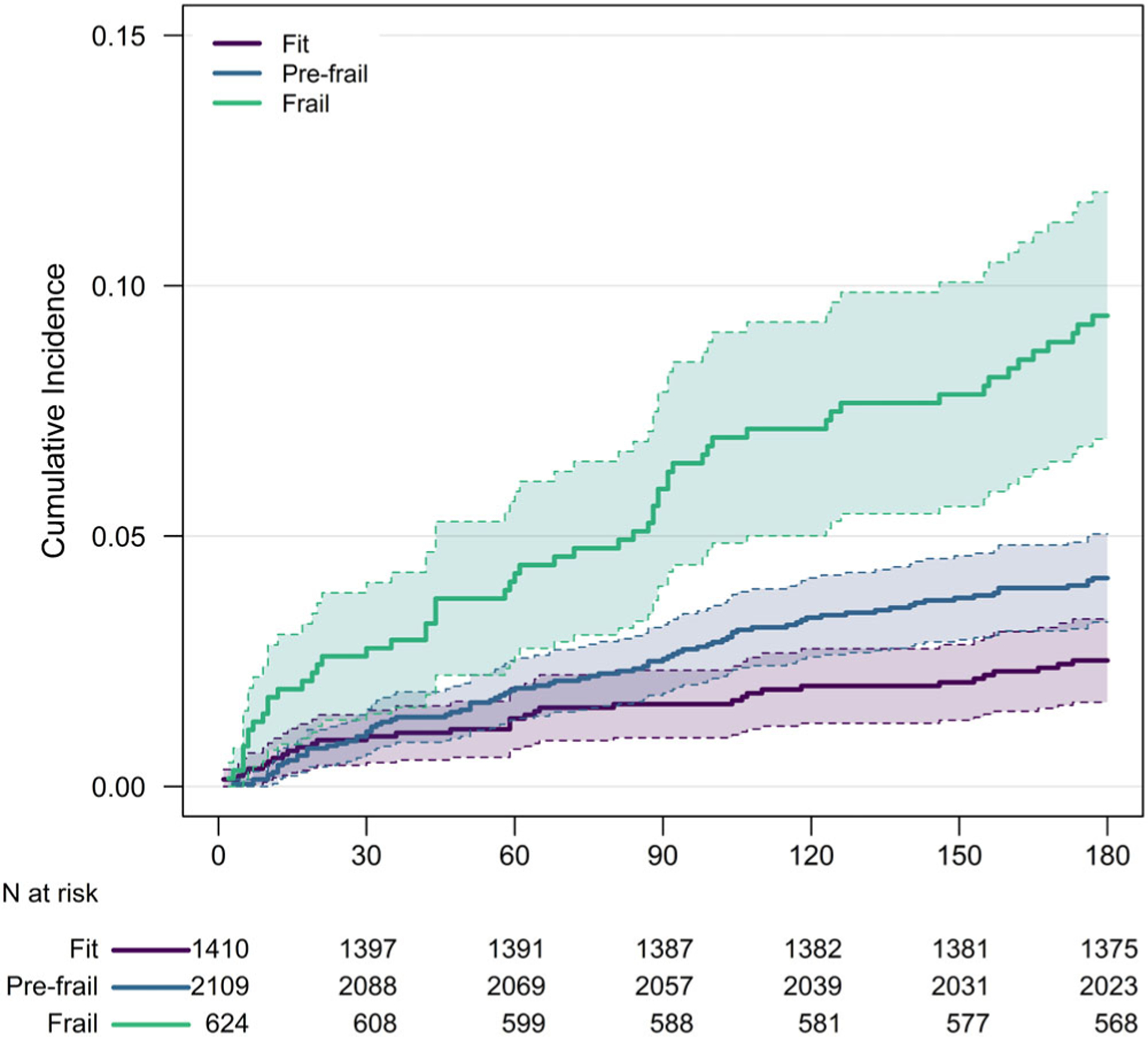
Of 4,831 unique patients (2,281 females (47.3%); mean (SD) age, 73.2 (5.9) years), 4,143 (85.7%) had sufficient EHR data to calculate the eFI, with 15.1% categorized as frail (eFI > 0.21) and 50.9% pre-frail (0.10 < eFI ≤ 0.21). For all outcomes, there was a generally a gradation of risk with higher eFI scores. For example, adjusting for age, sex, race/ethnicity, and American Society of Anesthesiologists class, and accounting for variability by service line, patients identified as frail based on the eFI, compared to fit patients, had greater needs for post-acute care (odds ratio (OR) = 1.68; 95% confidence interval (CI) = 1.36-2.08), higher rates of 30-day readmission (hazard ratio (HR) = 2.46; 95%CI = 1.72-3.52) and higher all-cause mortality (HR = 2.86; 95%CI = 1.84-4.44) over 6 months' follow-up.
The eFI, an automated digital marker for frailty integrated within the EHR, can facilitate pre-operative frailty screening at scale.
衰弱与老年人术后众多不良结局相关。当前的术前衰弱筛查工具需要额外的数据收集或客观评估,这增加了费用并限制了大规模应用。
评估电子健康记录(EHR)中整合的衰弱自动测量指标与非急诊手术术后结局之间的关联。
回顾性队列研究。
学术医疗中心。
2017年10月8日至2019年6月1日期间接受非急诊手术且住院时间达24小时或更长时间的65岁及以上患者。
通过54项电子衰弱指数(eFI)测量的衰弱情况。
住院时间、急性后期护理需求、30天再入院率和6个月全因死亡率。
在4831例独特患者中(2281例女性(47.3%);平均(标准差)年龄73.2(5.9)岁),4143例(85.7%)有足够的EHR数据来计算eFI,其中15.1%被归类为衰弱(eFI>0.21),50.9%为衰弱前期(0.10<eFI≤0.21)。对于所有结局,eFI得分越高,风险通常呈梯度变化。例如,在调整年龄、性别、种族/民族和美国麻醉医师协会分级,并考虑各业务线的变异性后,与健康患者相比,基于eFI被确定为衰弱的患者对急性后期护理的需求更大(优势比(OR)=1.68;95%置信区间(CI)=1.36 - 2.08),30天再入院率更高(风险比(HR)=2.46;95%CI = 1.72 - 3.52),且在6个月的随访期间全因死亡率更高(HR = 2.86;95%CI = 1.84 - 4.44)。
EHR中整合的eFI作为一种衰弱的自动数字标志物,可促进大规模的术前衰弱筛查。