Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts (H.A., R.K.L., R.P.R.).
Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts (S.G., D.E.L.).
Ann Intern Med. 2021 May;174(5):622-632. doi: 10.7326/M20-6739. Epub 2021 Jan 26.
Hypercoagulability may be a key mechanism of death in patients with coronavirus disease 2019 (COVID-19).
To evaluate the incidence of venous thromboembolism (VTE) and major bleeding in critically ill patients with COVID-19 and examine the observational effect of early therapeutic anticoagulation on survival.
In a multicenter cohort study of 3239 critically ill adults with COVID-19, the incidence of VTE and major bleeding within 14 days after intensive care unit (ICU) admission was evaluated. A target trial emulation in which patients were categorized according to receipt or no receipt of therapeutic anticoagulation in the first 2 days of ICU admission was done to examine the observational effect of early therapeutic anticoagulation on survival. A Cox model with inverse probability weighting to adjust for confounding was used.
67 hospitals in the United States.
Adults with COVID-19 admitted to a participating ICU.
Time to death, censored at hospital discharge, or date of last follow-up.
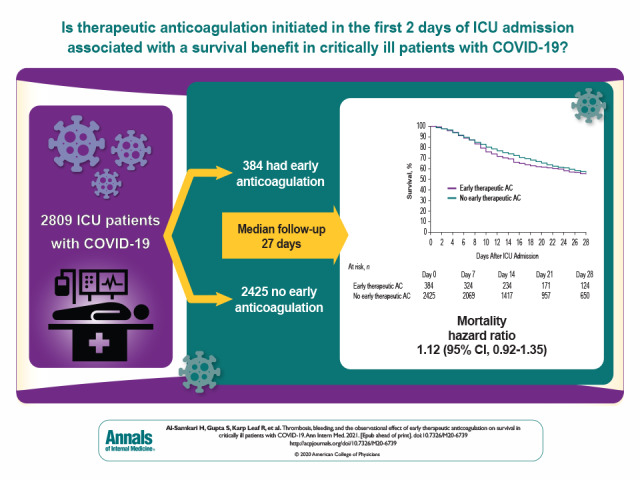
Among the 3239 patients included, the median age was 61 years (interquartile range, 53 to 71 years), and 2088 (64.5%) were men. A total of 204 patients (6.3%) developed VTE, and 90 patients (2.8%) developed a major bleeding event. Independent predictors of VTE were male sex and higher D-dimer level on ICU admission. Among the 2809 patients included in the target trial emulation, 384 (11.9%) received early therapeutic anticoagulation. In the primary analysis, during a median follow-up of 27 days, patients who received early therapeutic anticoagulation had a similar risk for death as those who did not (hazard ratio, 1.12 [95% CI, 0.92 to 1.35]).
Observational design.
Among critically ill adults with COVID-19, early therapeutic anticoagulation did not affect survival in the target trial emulation.
None.
高凝状态可能是 2019 年冠状病毒病(COVID-19)患者死亡的关键机制。
评估危重症 COVID-19 患者静脉血栓栓塞(VTE)和大出血的发生率,并研究早期治疗性抗凝对生存的观察效果。
在一项对 3239 例危重症 COVID-19 成年患者的多中心队列研究中,评估了 ICU 入院后 14 天内 VTE 和大出血的发生率。根据 ICU 入院前 2 天是否接受治疗性抗凝,对患者进行分类,进行目标试验模拟,以研究早期治疗性抗凝对生存的观察效果。采用逆概率加权 Cox 模型调整混杂因素。
美国 67 家医院。
入住参与 ICU 的 COVID-19 成年患者。
死亡时间,以出院或最后一次随访为截止日期。
在纳入的 3239 例患者中,中位年龄为 61 岁(四分位间距,53 岁至 71 岁),2088 例(64.5%)为男性。共有 204 例(6.3%)发生 VTE,90 例(2.8%)发生大出血事件。VTE 的独立预测因素为男性和 ICU 入院时更高的 D-二聚体水平。在目标试验模拟中纳入的 2809 例患者中,384 例(11.9%)接受了早期治疗性抗凝。在主要分析中,中位随访 27 天期间,接受早期治疗性抗凝的患者与未接受治疗性抗凝的患者死亡风险相似(风险比,1.12[95%CI,0.92 至 1.35])。
观察性设计。
在危重症 COVID-19 成年患者中,早期治疗性抗凝在目标试验模拟中并未影响生存。
无。