Nance Michael, Khazi Zain, Kaifi Jussuf, Avella Diego, Alnijoumi Mohammed, Davis Ryan, Bhat Ambarish
Department of Vascular and Interventional Radiology, School of Medicine, Columbia, Missouri, United States.
Department of Radiology, Division of Cardiothoracic Surgery, Columbia, Missouri, United States.
J Clin Imaging Sci. 2021 Feb 9;11:7. doi: 10.25259/JCIS_224_2020. eCollection 2021.
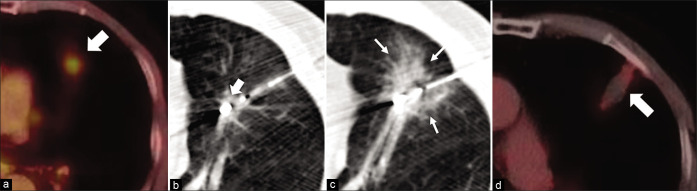
The objective of the study was to retrospectively investigate the safety and efficacy of computerized tomography-guided microwave ablation (MWA) in the treatment of Stage I non-small cell lung cancers (NSCLCs).
This retrospective, single-center study evaluated 21 patients (10 males and 11 females; mean age 73.8 ± 8.2 years) with Stage I peripheral NSCLCs treated with MWA between 2010 and 2020. All patients were surveyed for metastatic disease. Clinical success was defined as absence of FDG avidity on follow-up imaging. Tumor growth within 5 mm of the original ablated territory was defined as local recurrence. Welch -test and Fisher's exact test were used for univariate analysis. Hazard ratio (HR) and odds ratio (OR) were determined using Cox regression and Firth logistic regression. Significance was < 0.05. Data are expressed as mean ± standard deviation.
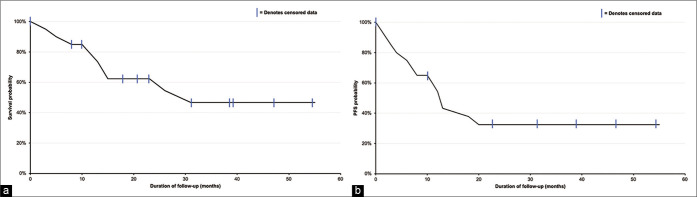
Ablated tumors had longest dimension 17.4 ± 5.4 mm and depth 19.7 ± 15.1 mm from the pleural surface. Median follow-up was 20 months (range, 0.6-56 months). Mean overall survival (OS) following lung cancer diagnosis or MWA was 26.2 ± 15.4 months (range, 5-56 months) and 23.7 ± 15.1 months (range, 3-55 months). OS at 1, 2, and 5 years was 67.6%, 61.8%, and 45.7%, respectively. Progression-free survival (PFS) was 19.1 ± 16.2 months (range, 1-55 months). PFS at 1, 2, and 5 years was 44.5%, 32.9%, and 32.9%, respectively. Technical success was 100%, while clinical success was observed in 95.2% (20/21) of patients. One patient had local residual disease following MWA and was treated with chemotherapy. Local control was 90% with recurrence in two patients following ablation. Six patients (28.6%) experienced post-ablation complications, with pneumothorax being the most common event (23.8% of patients). Female gender was associated with 90% reduction in risk of death (HR 0.1, = 0.014). Tumor longest dimension was associated with a 10% increase in risk of death ( = 0.197). Several comorbidities were associated with increased hazard. Univariate analysis revealed pre-ablation forced vital capacity trended higher among survivors (84.7 ± 15.2% vs. 73 ± 21.6%, = 0.093). Adjusted for age and sex, adenocarcinoma, and neuroendocrine histology trended toward improved OS (OR: 0.13, 0.13) and PFS (OR: 0.88, 0.37) compared to squamous cell carcinoma.
MWA provides a safe and effective alternative to stereotactic brachytherapy resulting in promising OS and PFS in patients with Stage I peripheral NSCLC. Larger sample sizes are needed to further define the effects of underlying comorbidities and tumor biology.
本研究的目的是回顾性调查计算机断层扫描引导下的微波消融(MWA)治疗Ⅰ期非小细胞肺癌(NSCLC)的安全性和有效性。
这项回顾性单中心研究评估了2010年至2020年间接受MWA治疗的21例Ⅰ期周围型NSCLC患者(10例男性和11例女性;平均年龄73.8±8.2岁)。对所有患者进行转移性疾病调查。临床成功定义为随访成像时无FDG摄取。在距原始消融区域5mm内的肿瘤生长定义为局部复发。采用韦尔奇检验和费舍尔精确检验进行单因素分析。使用Cox回归和Firth逻辑回归确定风险比(HR)和比值比(OR)。显著性水平为<0.05。数据以平均值±标准差表示。
消融肿瘤的最大直径为17.4±5.4mm,距胸膜表面的深度为19.7±15.1mm。中位随访时间为20个月(范围0.6 - 56个月)。肺癌诊断或MWA后的平均总生存期(OS)为26.2±15.4个月(范围5 - 56个月)和23.7±15.1个月(范围3 - 55个月)。1年、2年和5年的OS分别为67.6%、61.8%和45.7%。无进展生存期(PFS)为19.1±16.2个月(范围1 - 55个月)。1年、2年和5年的PFS分别为44.5%、32.9%和32.9%。技术成功率为100%,而95.2%(20/21)的患者观察到临床成功。1例患者MWA后有局部残留病灶并接受了化疗。局部控制率为90%,2例患者消融后复发。6例患者(28.6%)出现消融后并发症,气胸是最常见的事件(占患者的23.8%)。女性性别与死亡风险降低90%相关(HR 0.1,P = 0.014)。肿瘤最大直径与死亡风险增加10%相关(P = 0.197)。几种合并症与风险增加相关。单因素分析显示,消融前用力肺活量在幸存者中趋势较高(84.7±15.2%对73±21.6%,P = 0.093)。与鳞状细胞癌相比,在调整年龄、性别、腺癌和神经内分泌组织学后,OS(OR:0.13,0.13)和PFS(OR:0.88,0.37)有改善趋势。
MWA为立体定向近距离放射治疗提供了一种安全有效的替代方法,在Ⅰ期周围型NSCLC患者中产生了有前景的OS和PFS。需要更大的样本量来进一步确定潜在合并症和肿瘤生物学的影响。