Pawlowski Colin, Venkatakrishnan A J, Kirkup Christian, Berner Gabriela, Puranik Arjun, O'Horo John C, Badley Andrew D, Soundararajan Venky
nference inc., One Main Street, Suite 400, East Arcade, Cambridge, MA 02142, USA.
Mayo Clinic, Rochester, MN, USA.
EClinicalMedicine. 2021 Mar;33:100774. doi: 10.1016/j.eclinm.2021.100774. Epub 2021 Mar 9.
Coagulopathies are a major class among COVID-19 associated complications. Although anticoagulants such as unfractionated Heparin and Enoxaparin are both being used for therapeutic mitigation of COVID associated coagulopathy (CAC), differences in their clinical outcomes remain to be investigated.
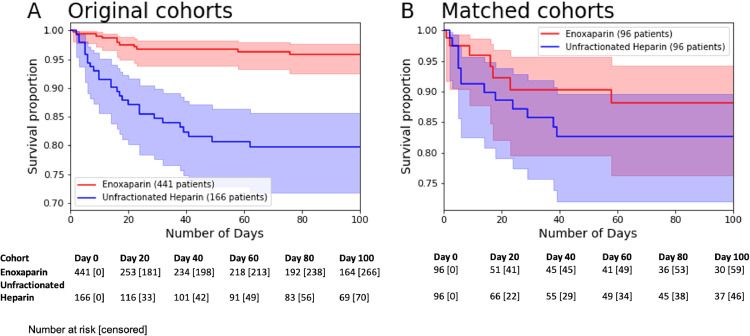
We analyzed records of 1,113 patients in the Mayo Clinic Electronic Health Record (EHR) database who were admitted to the hospital for COVID-19 between April 4, 2020 and August 31, 2020, including 19 different Mayo Clinic sites in Arizona, Florida, Minnesota, and Wisconsin. Among this patient population, we compared cohorts of patients who received different types of anticoagulants, including 441 patients who received unfractionated Heparin and 166 patients who received Enoxaparin. Clinical outcomes at 28 days were compared, and propensity score matching was used to control for potential confounding variables including: demographics, comorbidities, ICU status, chronic kidney disease stage, and oxygenation status. Patients with a history of acute kidney injury and patients who received multiple types of anticoagulants were excluded from the study.
We find that COVID-19 patients administered unfractionated Heparin but not Enoxaparin have higher rates of 28-day mortality (risk ratio: 4.3; 95% Confidence Interval [C.I.].: [1.8, 10.2]; -value: 8.5e-4, Benjamini Hochberg [BH] adjusted -value: 2.1e-3), after controlling for potential confounding factors.
This study emphasizes the need for mechanistically investigating differential modulation of the COVID-associated coagulation cascades by Enoxaparin versus unfractionated Heparin.
This work was supported by Nference, inc.
凝血功能障碍是新冠病毒病(COVID-19)相关并发症中的一个主要类别。尽管普通肝素和依诺肝素等抗凝剂都被用于治疗缓解新冠病毒相关凝血功能障碍(CAC),但其临床疗效差异仍有待研究。
我们分析了梅奥诊所电子健康记录(EHR)数据库中2020年4月4日至2020年8月31日期间因COVID-19入院的1113例患者的记录,这些患者来自亚利桑那州、佛罗里达州、明尼苏达州和威斯康星州的19个不同的梅奥诊所站点。在这一患者群体中,我们比较了接受不同类型抗凝剂治疗的患者队列,包括441例接受普通肝素治疗的患者和166例接受依诺肝素治疗的患者。比较了28天时的临床结局,并采用倾向评分匹配法来控制潜在的混杂变量,包括:人口统计学特征、合并症、重症监护病房(ICU)状态、慢性肾脏病分期和氧合状态。有急性肾损伤病史的患者和接受多种类型抗凝剂治疗的患者被排除在研究之外。
我们发现,在控制潜在混杂因素后,接受普通肝素而非依诺肝素治疗的COVID-19患者28天死亡率更高(风险比:4.3;95%置信区间[C.I.]:[1.8, 10.2];P值:8.5e-4,经本雅明尼-霍奇伯格[BH]校正的P值:2.1e-3)。
本研究强调有必要从机制上研究依诺肝素与普通肝素对新冠病毒相关凝血级联反应的不同调节作用。
本研究得到了Nference公司的支持。