Hovanesian John A, Nichols Kelly K, Jackson Mitchell, Katz James, Chan Arthur, Glassberg Mrudula B, Sloesen Brigitte, Korves Caroline, Nguyen Catherine, Syntosi Annie
Harvard Eye Associates, Laguna Hills, CA, USA.
UCLA Jules Stein Eye Institute, Los Angeles, CA, USA.
Clin Ophthalmol. 2021 Mar 8;15:1041-1054. doi: 10.2147/OPTH.S296510. eCollection 2021.
This study evaluated real-world treatment of dry eye disease (DED) with lifitegrast.
Ophthalmologists and optometrists treating patients with DED were invited to participate through a healthcare provider (HCP)-based panel. HCPs completed a provider survey and contributed data toward a chart review for up to five qualifying patients with DED who initiated lifitegrast ophthalmic solution (index date) between 01/01/2017 (US) or 01/01/2018 (Canada) and 06/30/2019. Patient demographics, treatments, clinical characteristics, and outcomes (ie, severity, signs, symptoms) were collected for the 6-month pre-index period and up to 12-months post-index.
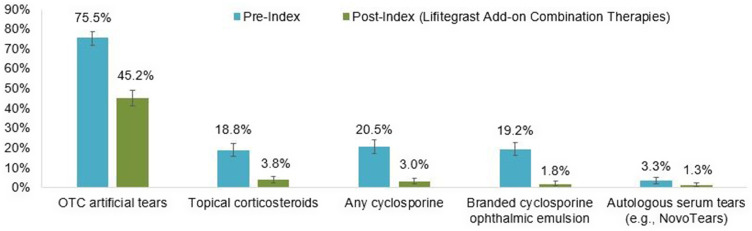
For this study, 517 HCPs contributed 600 patient charts. Among 554 and 281 patients with follow-up at 6 and 12-months post-index, 512 (92.4%) and 238 (84.7%) patients had ongoing lifitegrast treatment, respectively. Other DED-related treatments were less frequently used post-index with lifitegrast vs pre-index: over-the-counter artificial tear use (45.2% vs 75.5%), topical corticosteroids (3.8% vs 18.8%), any cyclosporine (3.0% vs 20.5%). At 3-months (n=571) and 12-months (n=320) post-index vs pre-index, fewer patients had eye dryness (47 [8.2%] and 16 [5.0%] vs 525 [87.5%]), blurred vision (28 [4.9%] and 11 [3.4%] vs 346 [57.7%]), ocular burning/stinging (25 [4.4%] and 8 [2.5%] vs 336 [56.0%]), depression (8 [1.4%] and 9 [2.8%] vs 55 [9.2%]), fatigue (4 [0.7%] and 1 [0.3%] vs 82 [13.7%]), and headache (1 [0.2%] and 0 vs 19 [3.2%]). At 3 and 12-months post-index vs pre-index, average corneal staining score was numerically lower (2.7 and 2.0 vs 6.5), and average Schirmer score (10.6 and 10 vs 6.3) and tear film break-up time (7.3 and 8.0 vs 4.8) higher.
The majority of patients had ongoing lifitegrast treatment 6-months post-index with reduction in overall treatment burden. Improvement in DED signs and symptoms, including QoL impacts, was evident at 3 months and up to 12 months after lifitegrast initiation.
本研究评估了lifitegrast在干眼症(DED)实际治疗中的应用。
通过基于医疗服务提供者(HCP)的小组邀请治疗DED患者的眼科医生和验光师参与。HCP完成一份提供者调查问卷,并为截至2019年6月30日期间,在2017年1月1日(美国)或2018年1月1日(加拿大)至2019年6月30日开始使用lifitegrast眼药水(索引日期)的最多五名符合条件的DED患者的病历审查提供数据。收集患者在索引前6个月和索引后长达12个月的人口统计学、治疗、临床特征和结果(即严重程度、体征、症状)。
在本研究中,517名HCP提供了600份患者病历。在索引后6个月和12个月有随访的554名和281名患者中,分别有512名(92.4%)和238名(84.7%)患者持续接受lifitegrast治疗。与索引前相比,索引后使用lifitegrast时其他与DED相关的治疗使用频率较低:非处方人工泪液使用(45.2%对75.5%)、局部用皮质类固醇(3.8%对18.8%)、任何环孢素(3.0%对20.5%)。与索引前相比,索引后3个月(n = 571)和12个月(n = 320)时,有眼干症状的患者更少(47例[8.2%]和16例[5.0%]对525例[87.5%])、视力模糊(28例[4.9%]和11例[3.4%]对346例[57.7%])、眼部灼烧/刺痛(25例[4.4%]和8例[2.5%]对336例[56.0%])、抑郁(8例[1.4%]和9例[2.8%]对55例[9.2%])、疲劳(4例[0.7%]和1例[0.3%]对82例[13.7%])以及头痛(1例[0.2%]和0例对19例[3.2%])。与索引前相比,索引后3个月和12个月时,平均角膜染色评分在数值上更低(2.7和2.0对6.5),平均泪液分泌试验评分(10.6和10对6.3)和泪膜破裂时间(7.3和8.0对4.8)更高。
大多数患者在索引后6个月持续接受lifitegrast治疗,总体治疗负担减轻。在开始使用lifitegrast后3个月至12个月,DED的体征和症状包括对生活质量的影响均有明显改善。