Ravera Alice, Santema Bernadet T, Sama Iziah E, Meyer Sven, Lombardi Carlo M, Carubelli Valentina, Ferreira João Pedro, Lang Chim C, Dickstein Kenneth, Anker Stefan D, Samani Nilesh J, Zannad Faiez, van Veldhuisen Dirk J, Teerlink John R, Metra Marco, Voors Adriaan A
Institute of Cardiology, ASST Spedali Civili di Brescia and Department of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, Brescia, Italy.
Department of Cardiology, University of Groningen, Groningen, The Netherlands.
Eur J Heart Fail. 2021 Apr;23(4):567-577. doi: 10.1002/ejhf.2154. Epub 2021 May 4.
We sought to analyse quality of life (QoL) measures derived from two questionnaires widely used in clinical trials, the Kansas City Cardiomyopathy Questionnaire (KCCQ) and the EuroQoL 5 dimensions (EQ-5D), and to compare their prognostic value in men and women with heart failure and reduced ejection fraction (HFrEF).
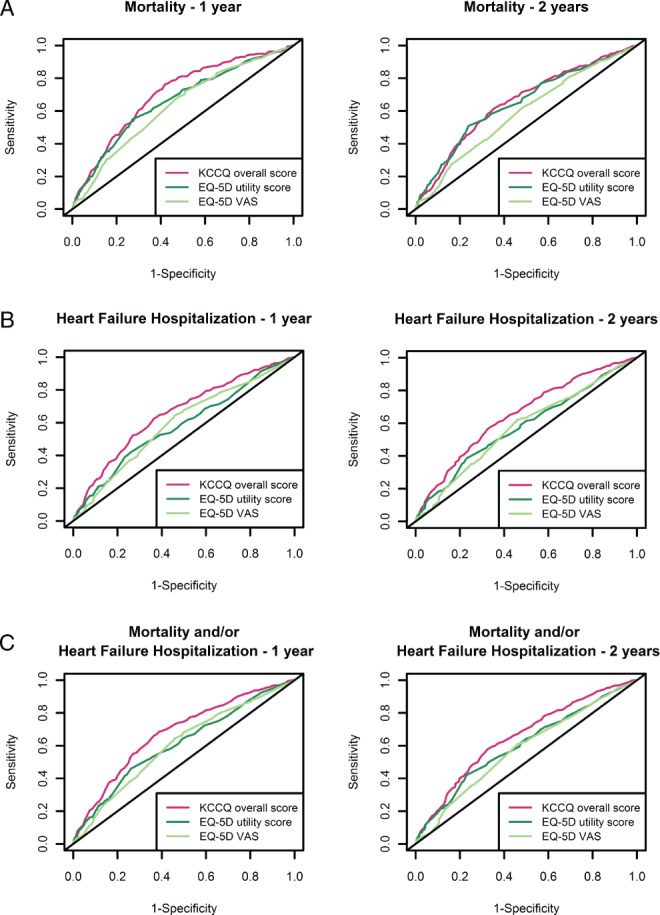
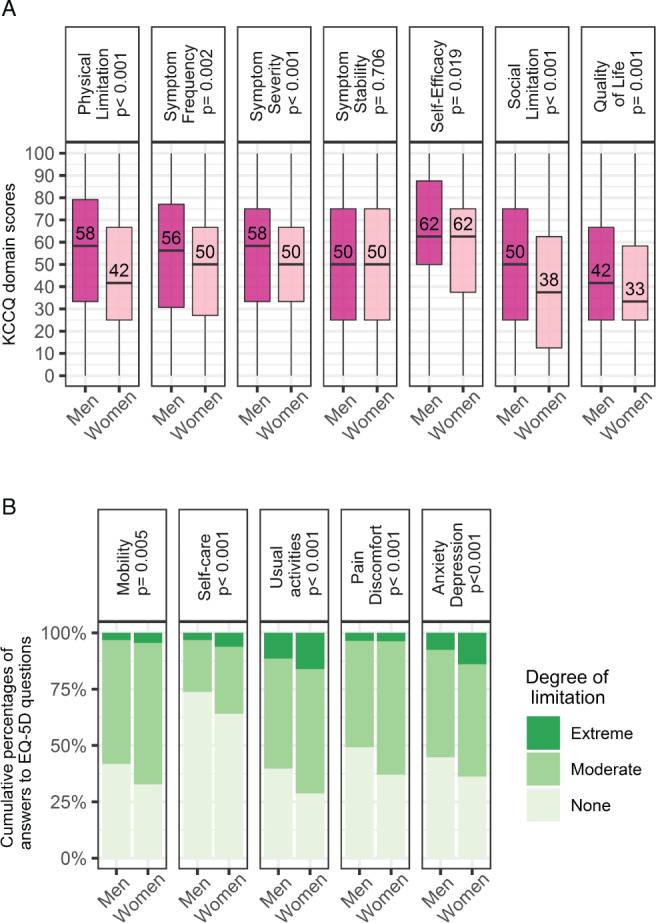
From the BIOlogy Study to TAilored Treatment in Chronic Heart Failure (BIOSTAT-CHF) we compared KCCQ and EQ-5D at baseline and after 9 months in 1276 men and 373 women with new-onset or worsening symptoms of HFrEF, who were sub-optimally treated and in whom there was an anticipated up-titration of guideline-derived medical therapies. Women had significantly worse baseline QoL (median) as compared with men, both when assessed with KCCQ overall score (KCCQ-OS, 44 vs. 53, P < 0.001) and EQ-5D utility score (0.62 vs. 0.73, P < 0.001). QoL improved equally in women and men at follow-up. All summary measures of QoL were independently associated with all-cause mortality, with KCCQ-OS showing the most remarkable association with mortality up to 1 year compared to the EQ-5D scores (C-statistic 0.650 for KCCQ-OS vs. 0.633 and 0.599 for EQ-5D utility score and EQ-5D visual analogue scale, respectively). QoL was associated with all outcomes analysed, both in men and women (all P for interaction with sex >0.2).
Amongst patients with HFrEF, women reported significantly worse QoL than men. QoL was independently associated with subsequent outcome, similarly in men and women. The KCCQ in general, and the KCCQ-OS in particular, showed the strongest independent association with outcome.
我们试图分析源自两项广泛用于临床试验的问卷(堪萨斯城心肌病问卷(KCCQ)和欧洲五维健康量表(EQ-5D))的生活质量(QoL)测量方法,并比较它们在射血分数降低的心力衰竭(HFrEF)男性和女性中的预后价值。
在慢性心力衰竭生物研究以实现个体化治疗(BIOSTAT-CHF)中,我们比较了1276名男性和373名女性新发或症状恶化的HFrEF患者在基线时以及9个月后的KCCQ和EQ-5D,这些患者治疗未达最佳,且预期会增加基于指南的药物治疗剂量。与男性相比,女性的基线QoL(中位数)显著更差,无论是用KCCQ总分(KCCQ-OS,44对53,P<0.001)还是EQ-5D效用评分(0.62对0.73,P<0.001)评估时均如此。随访时男性和女性的QoL改善程度相同。所有QoL汇总指标均与全因死亡率独立相关,与EQ-5D评分相比,KCCQ-OS在长达1年的时间里与死亡率的关联最为显著(KCCQ-OS的C统计量为0.650,而EQ-5D效用评分和EQ-5D视觉模拟量表分别为0.633和0.599)。QoL与分析的所有结局相关,在男性和女性中均如此(所有性别交互作用的P值>0.2)。
在HFrEF患者中,女性报告的QoL显著低于男性。QoL与随后的结局独立相关,在男性和女性中情况相似。总体而言,KCCQ,尤其是KCCQ-OS,与结局的独立关联最强。