Department of Non-communicable Disease Epidemiology, Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK.
Department of Quality Measurements and Research, Clalit Health Services, Tel Aviv, Israel.
Br J Dermatol. 2021 Oct;185(4):772-780. doi: 10.1111/bjd.20067. Epub 2021 Jun 6.
Emerging evidence suggests an association between common inflammatory skin diseases and chronic kidney disease (CKD).
To explore the association between CKD stages 3-5 (CKD3-5) and atopic eczema, psoriasis, rosacea and hidradenitis suppurativa.
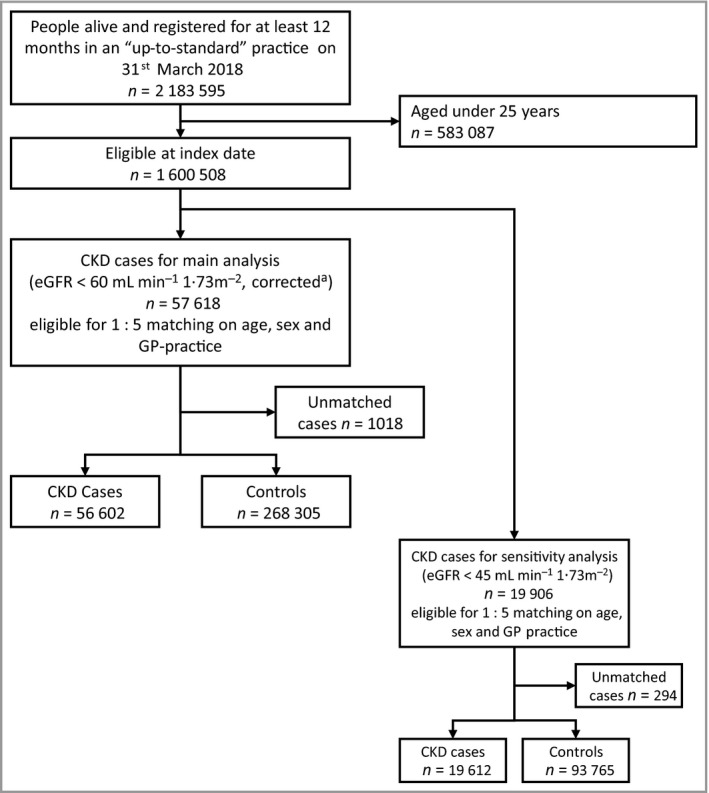
We undertook two complementary analyses; a prevalent case-control study and a cohort study using routinely collected primary care data [UK Clinical Practice Research Datalink (CPRD)]. We matched individuals with CKD3-5 in CPRD in March 2018 with up to five individuals without CKD for general practitioner practice, age and sex. We compared the prevalence of CKD3-5 among individuals with and without each inflammatory skin disease. We included individuals in CPRD with diabetes mellitus (2004-2018) in a cohort analysis to compare the incidence of CKD3-5 among people with and without atopic eczema and psoriasis.
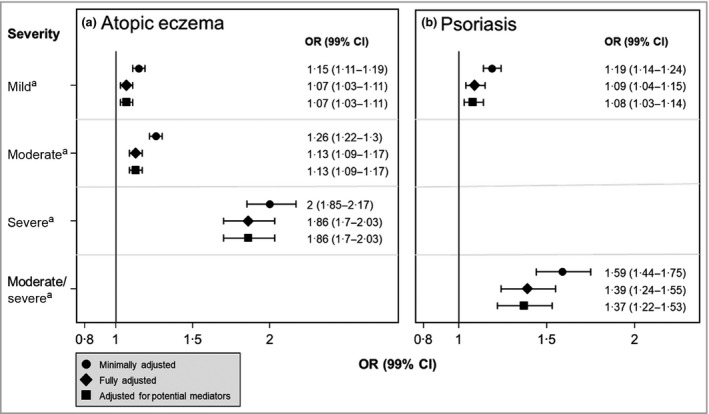
Our study included 56 602 cases with CKD3-5 and 268 305 controls. Cases were more likely than controls to have a history of atopic eczema [odds ratio (OR) 1·14, 99% confidence interval (CI) 1·11-1·17], psoriasis (OR 1·13, 99% CI 1·08-1·19) or hidradenitis suppurativa (OR 1·49, 99% CI 1·19-1·85), but were slightly less likely to have been diagnosed with rosacea (OR 0·92, 99% CI 0·87-0·97), after adjusting for age, sex, practice (matching factors), index of multiple deprivation, diabetes, smoking, harmful alcohol use and obesity. Results remained similar after adjusting for hypertension and cardiovascular disease. In the cohort with diabetes (N = 335 827), there was no evidence that CKD3-5 incidence was associated with atopic eczema or psoriasis.
Atopic eczema, psoriasis and hidradenitis suppurativa are weakly associated with CKD3-5. Future research is needed to elucidate potential mechanisms and the clinical significance of our findings.
新出现的证据表明,常见的炎症性皮肤病与慢性肾脏病(CKD)之间存在关联。
探讨 CKD3-5 期(CKD3-5)与特应性皮炎、银屑病、酒渣鼻和化脓性汗腺炎之间的关系。
我们进行了两项互补分析;一项基于常规收集的初级保健数据的现患病例对照研究和队列研究[英国临床实践研究数据链接(CPRD)]。我们在 2018 年 3 月将 CPRD 中的 CKD3-5 患者与同一全科医生诊所、年龄和性别相匹配的不伴有 CKD 的 5 名个体进行匹配。我们比较了伴有和不伴有每种炎症性皮肤病的 CKD3-5 患者的患病率。我们将 CPRD 中患有糖尿病(2004-2018 年)的患者纳入队列分析,以比较特应性皮炎和银屑病患者中 CKD3-5 的发生率。
我们的研究包括 56602 例 CKD3-5 患者和 268305 例对照。病例组比对照组更有可能患有特应性皮炎[比值比(OR)1.14,99%置信区间(CI)1.11-1.17]、银屑病(OR 1.13,99%CI 1.08-1.19)或化脓性汗腺炎(OR 1.49,99%CI 1.19-1.85),但被诊断患有酒渣鼻的可能性略低(OR 0.92,99%CI 0.87-0.97),调整年龄、性别、实践(匹配因素)、多种剥夺指数、糖尿病、吸烟、有害饮酒和肥胖后。调整高血压和心血管疾病后,结果仍然相似。在患有糖尿病的队列中(N=335827),没有证据表明 CKD3-5 的发生率与特应性皮炎或银屑病有关。
特应性皮炎、银屑病和化脓性汗腺炎与 CKD3-5 有弱相关性。需要进一步研究以阐明我们研究结果的潜在机制和临床意义。