Brighton and Sussex Medical School, Brighton, United Kingdom.
Department of Clinical & Experimental Medicine, Faculty of Health Sciences, University of Surrey, Guildford, United Kingdom.
PLoS One. 2021 Mar 18;16(3):e0248477. doi: 10.1371/journal.pone.0248477. eCollection 2021.
Demographic changes alongside medical advances have resulted in older adults accounting for an increasing proportion of emergency hospital admissions. Current measures of illness severity, limited to physiological parameters, have shortcomings in this cohort, partly due to patient complexity. This study aimed to derive and validate a risk score for acutely unwell older adults which may enhance risk stratification and support clinical decision-making.
Data was collected from emergency admissions in patients ≥65 years from two UK general hospitals (April 2017- April 2018). Variables underwent regression analysis for in-hospital mortality and independent predictors were used to create a risk score. Performance was assessed on external validation. Secondary outcomes included seven-day mortality and extended hospital stay.
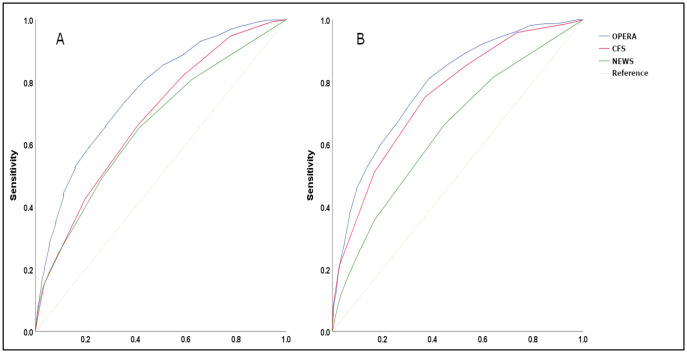
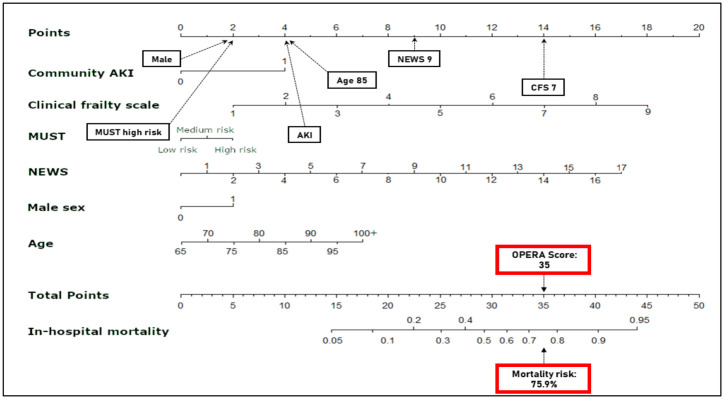
Derivation (n = 8,974) and validation (n = 8,391) cohorts were analysed. The model included the National Early Warning Score 2 (NEWS2), clinical frailty scale (CFS), acute kidney injury, age, sex, and Malnutrition Universal Screening Tool. For mortality, area under the curve for the model was 0.79 (95% CI 0.78-0.80), superior to NEWS2 0.65 (0.62-0.67) and CFS 0.76 (0.74-0.77) (P<0.0001). Risk groups predicted prolonged hospital stay: the highest risk group had an odds ratio of 9.7 (5.8-16.1) to stay >30 days.
Our simple validated model (Older Persons' Emergency Risk Assessment [OPERA] score) predicts in-hospital mortality and prolonged length of stay and could be easily integrated into electronic hospital systems, enabling automatic digital generation of risk stratification within hours of admission. Future studies may validate the OPERA score in external populations and consider an impact analysis.
人口结构变化和医学进步导致老年患者在急诊入院患者中的比例不断增加。目前的疾病严重程度评估方法仅限于生理参数,在这一人群中存在缺陷,部分原因是患者病情复杂。本研究旨在为病情急危的老年患者开发和验证一种风险评分,以增强风险分层,并为临床决策提供支持。
本研究的数据来自于 2017 年 4 月至 2018 年 4 月期间英国两家综合医院的老年(≥65 岁)急诊入院患者。对入院患者的变量进行回归分析,确定院内死亡率的独立预测因素,并据此建立风险评分。通过外部验证评估其性能。次要结局包括 7 天死亡率和延长住院时间。
对 8974 名患者进行了推导,对 8391 名患者进行了验证。该模型纳入了国家早期预警评分 2(NEWS2)、临床虚弱量表(CFS)、急性肾损伤、年龄、性别和营养不良通用筛查工具。对于死亡率,该模型的曲线下面积为 0.79(95%CI 0.78-0.80),优于 NEWS2 的 0.65(0.62-0.67)和 CFS 的 0.76(0.74-0.77)(P<0.0001)。风险组预测延长住院时间:风险最高的组住院时间超过 30 天的比值比为 9.7(5.8-16.1)。
我们的验证后的简单模型(老年人急诊风险评估[OPERA]评分)可以预测院内死亡率和延长住院时间,并且可以很容易地整合到电子医院系统中,在入院数小时内自动生成风险分层。未来的研究可能会在外部人群中验证 OPERA 评分,并考虑进行影响分析。