Centre for Economic and Social Research on Dementia, National University of Ireland Galway, Newcastle Road, Galway, H91 TK33, Ireland.
Institute of Mental Health, University of Nottingham, Nottingham, NG7 2RD, UK.
BMC Health Serv Res. 2021 Mar 18;21(1):243. doi: 10.1186/s12913-021-06230-9.
The understanding of appropriate or optimal care is particularly important for dementia, characterised by multiple, long-term, changing needs and the increasing expectations of people using services. However, the response of health and social care services is limited by resource constraints in most countries. This study sought to determine the optimal level, mix and cost of services for different dementia case types across the dementia continuum, and to better understand the resource allocation decision making process among health and social care professionals (HSCPs).
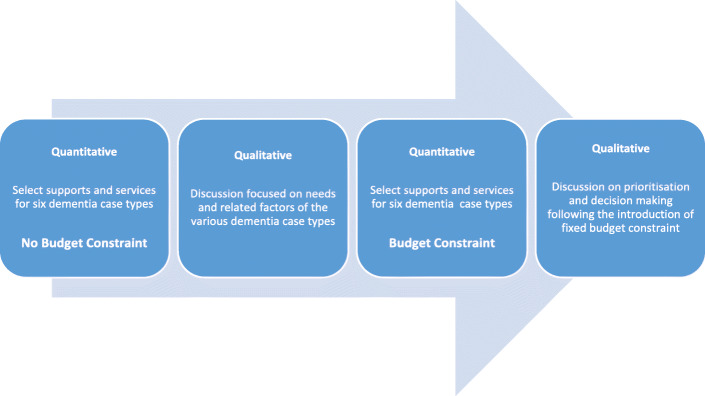
A balance of care framework was applied to the study questions and developed in three ways; firstly by considering optimality across the course of dementia and not just at the margin with residential care; secondly, through the introduction of a fixed budget to reveal constrained optimisation strategies; and thirdly through the use of a mixed methods design whereby qualitative data was collected at workshops using nominal group technique and analysed to obtain a more detailed understanding of the decision-making process. Twenty four HSCPs from a variety of disciplines participated in the resource allocation decision-making exercise.
HSCPs differentiated between case type severity; providing 2.6 times more resources to case types with higher level needs than those with lower level needs. When a resource constraint was introduced there was no evidence of any disproportionate rationing of services on the basis of need, i.e. more severe case types were not favoured over less severe case types. However, the fiscal constraint led to a much greater focus on meeting physical and clinical dependency needs through conventional social care provision. There was less emphasis on day care and psychosocial provision when resources were scarcer following the introduction of a fixed budget constraint.
HSCPs completed complex resource allocation exercises for people with dementia, including expected differentiation across case type severity. When rationing was introduced, HSCPs did not discriminate in favour of case types with high levels of need. They did, however, support conventional home care provision over psychosocial care, although participants were still keen to provide some residual cover for the latter, especially for case types that might benefit.
对于痴呆症,理解适当或最佳的护理特别重要,因为它具有多种、长期、不断变化的需求,以及服务使用者的期望不断增加。然而,在大多数国家,卫生和社会保健服务的反应受到资源限制的限制。本研究旨在确定不同痴呆病例类型在痴呆连续体中的最佳服务水平、组合和成本,并更好地了解卫生和社会保健专业人员(HSCPs)的资源分配决策过程。
平衡护理框架应用于研究问题,并通过三种方式进行开发;首先,考虑到痴呆症过程中的最优性,而不仅仅是在有住宿护理的边缘;其次,通过引入固定预算来揭示受限制的优化策略;最后,通过使用混合方法设计,在使用名义团体技术的研讨会上收集定性数据,并进行分析,以获得对决策过程的更详细了解。来自各种学科的 24 名 HSCP 参与了资源分配决策制定练习。
HSCP 区分了病例类型的严重程度;为需求水平较高的病例类型提供的资源是需求水平较低的病例类型的 2.6 倍。当引入资源限制时,没有证据表明根据需要进行任何不成比例的服务配给,即更严重的病例类型不会优先于不太严重的病例类型。然而,在引入固定预算限制后,资源更加稀缺,这导致更多地关注通过传统社会护理来满足身体和临床依赖需求。当资源稀缺时,对日间护理和心理社会服务的重视程度降低。
HSCP 为痴呆症患者完成了复杂的资源分配练习,包括根据病例类型严重程度进行预期的区分。当进行配给时,HSCP 并没有偏向于需求水平高的病例类型。然而,他们确实支持传统的家庭护理,而不是心理社会护理,尽管参与者仍然热衷于为后者提供一些剩余的覆盖,特别是对于可能受益的病例类型。