Fylan Beth, Ismail Hanif, Hartley Suzanne, Gale Chris P, Farrin Amanda J, Gardner Peter, Silcock Jonathan, Alldred David P
School of Pharmacy and Medical Sciences, University of Bradford, Richmond Road, Bradford, BD7 1DP, UK.
NIHR Yorkshire and Humber Patient Safety Translational Research Centre. Bradford Institute for Health Research, Temple Bank House, Bradford, BD9 6RJ, UK.
Pilot Feasibility Stud. 2021 Mar 26;7(1):85. doi: 10.1186/s40814-021-00819-x.
Heart failure affects 26 million people globally, and the optimal management of medicines is crucial for patients, particularly when their care is transferred between hospital and the community. Optimising clinical outcomes requires well-calibrated cross-organisational processes with staff and patients responding and adapting to medicines changes. The aim of this study was to assess the feasibility of implementing a complex intervention (the Medicines at Transitions Intervention; MaTI) co-designed by patients and healthcare staff. The purpose of the intervention was to optimise medicines management across the gaps between secondary and primary care when hospitals handover care. The study objectives were to (1) assess feasibility through meeting specified progression criteria to proceed to the trial, (2) assess if the intervention was acceptable to staff and patients, and (3) determine whether amendment or refinement would be needed to enhance the MaTI.
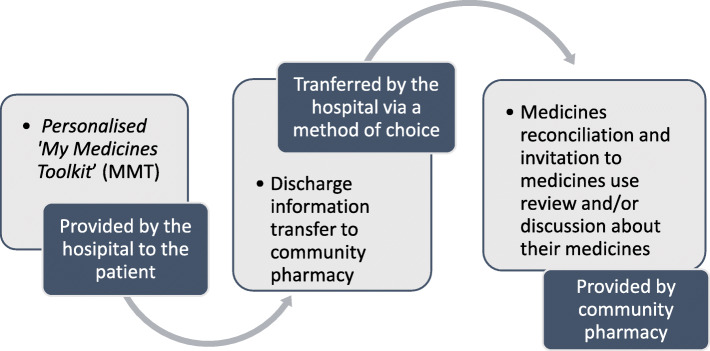
The feasibility of the MaTI was tested in three healthcare areas in the North of England between July and October 2017. Feasibility was measured and assessed through four agreed progression to trial criteria: (1) patient recruitment, (2) patient receipt of a medicines toolkit, (3) transfer of discharge information to community pharmacy, and (4) offer of a community pharmacy medicines review/discussion or medicines reconciliation. From the cardiology wards at each of the three NHS Acute Trusts (sites), 10 patients (aged ≥ 18 years) were recruited and introduced to the 'My Medicines Toolkit' (MMT). Patients were asked to identify their usual community pharmacy or nominate a pharmacy. Discharge information was transferred to the community pharmacy; pharmacists were asked to reconcile medicines and invited patients for a medicines use review (MUR) or discussion. At 1 month following discharge, all patients were sent three questionnaire sets: quality-of-life, healthcare utilisation, and a patient experience survey. In a purposive sample, 20 patients were invited to participate in a semi-structured interview about their experiences of the MaTI. Staff from hospital and primary care settings involved in patients' care were invited to participate in a semi-structured interview. Patient and staff interviews were analysed using Framework Analysis. Questionnaire completion rates were recorded and data were descriptively analysed.
Thirty-one patients were recruited across three sites. Eighteen staff and 18 patients took part in interviews, and 19 patients returned questionnaire sets. All four progression to trial criteria were met. We identified barriers to patient engagement with the intervention in hospital, which were compounded by patients' focus on returning home. Some patients described not engaging in discussions with staff about medicines and lacking motivation to do so because they were preoccupied with returning home. Some patients were unable or unwilling to attend a community pharmacy in person for a medicines review. Roles and responsibilities for delivering the MaTI were different in the three sites, and staff reported variations in time spent on MaTI activities. Staff reported some work pressures and staff absences that limited the time they could spend talking to patients about their medicines. Clinical teams reported that recording a target dose for heart failure medicines in patient-held documentation was difficult as they did not always know the ideal or tolerable dose. The majority of patients reported receiving the patient-held documentation. More than two-thirds reported being offered a MUR by their community pharmacists.
Delivery of the Medicines at Transitions Intervention (MaTI) was feasible at all three sites, and progression to trial criteria were met. Refinements were found to be necessary to overcome identified barriers and strengthen delivery of all steps of the intervention. Necessary changes to the MaTI were identified along with amendments to the implementation plan for the subsequent trial. Future implementation needs to take into account the complexity of medicines management and adaptation to local context.
心力衰竭影响着全球2600万人,药物的优化管理对患者至关重要,尤其是在其护理从医院转至社区期间。优化临床结果需要组织间流程得到良好校准,工作人员和患者能够对药物变化做出反应并进行调整。本研究的目的是评估实施一项由患者和医护人员共同设计的复杂干预措施(过渡用药干预措施;MaTI)的可行性。该干预措施的目的是在医院交接护理时优化二级和初级护理之间的药物管理。研究目标包括:(1)通过满足特定的进展标准来评估进行试验的可行性;(2)评估该干预措施对工作人员和患者是否可接受;(3)确定是否需要修正或完善MaTI以进行改进。
2017年7月至10月期间,在英格兰北部的三个医疗保健区域对MaTI的可行性进行了测试。通过四个商定的试验进展标准来衡量和评估可行性:(1)患者招募;(2)患者收到药物工具包;(3)将出院信息转交给社区药房;(4)提供社区药房药物审查/讨论或药物调和服务。从三个国民保健服务急性信托机构(研究地点)的心脏病病房中招募了10名年龄≥18岁的患者,并向他们介绍了“我的药物工具包”(MMT)。要求患者确定其常用的社区药房或指定一家药房。出院信息被转交给社区药房;药剂师被要求进行药物调和,并邀请患者进行药物使用审查(MUR)或讨论。出院后1个月,向所有患者发送了三套问卷:生活质量问卷、医疗保健利用问卷和患者体验调查问卷。在一个有目的的样本中,邀请了20名患者参加关于他们MaTI体验的半结构化访谈。邀请参与患者护理的医院和初级护理机构的工作人员参加半结构化访谈。使用框架分析法对患者和工作人员的访谈进行分析。记录问卷完成率,并对数据进行描述性分析。
在三个研究地点共招募了31名患者。18名工作人员和18名患者参加了访谈,19名患者返回了问卷。所有四个试验进展标准均得到满足。我们发现患者在医院参与该干预措施存在障碍,而患者对回家的关注使这些障碍更加复杂。一些患者表示没有与工作人员就药物进行讨论,也缺乏这样做的动力,因为他们一心想着回家。一些患者无法或不愿意亲自前往社区药房进行药物审查。在三个研究地点,实施MaTI的角色和职责各不相同,工作人员报告在MaTI活动上花费的时间也存在差异。工作人员报告了一些工作压力和人员缺勤情况,这限制了他们与患者谈论药物的时间。临床团队报告称,在患者持有的文件中记录心力衰竭药物的目标剂量很困难,因为他们并不总是知道理想或可耐受的剂量。大多数患者报告收到了患者持有的文件。超过三分之二的患者报告社区药剂师为他们提供了MUR。
在所有三个研究地点实施过渡用药干预措施(MaTI)都是可行的,并且满足了试验进展标准。发现有必要进行改进,以克服已识别的障碍并加强干预措施所有步骤的实施。确定了对MaTI的必要更改以及对后续试验实施计划的修正。未来的实施需要考虑药物管理的复杂性以及对当地情况的适应性。