Department of Old age Psychiatry, Division of Academic Psychiatry, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom.
Department of Psychosis Studies, Division of Academic Psychiatry, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom.
PLoS Med. 2021 Mar 29;18(3):e1003524. doi: 10.1371/journal.pmed.1003524. eCollection 2021 Mar.
Cannabinoid-based medicines (CBMs) are being used widely in the elderly. However, their safety and tolerability in older adults remains unclear. We aimed to conduct a systematic review and meta-analysis of safety and tolerability of CBMs in adults of age ≥50 years.
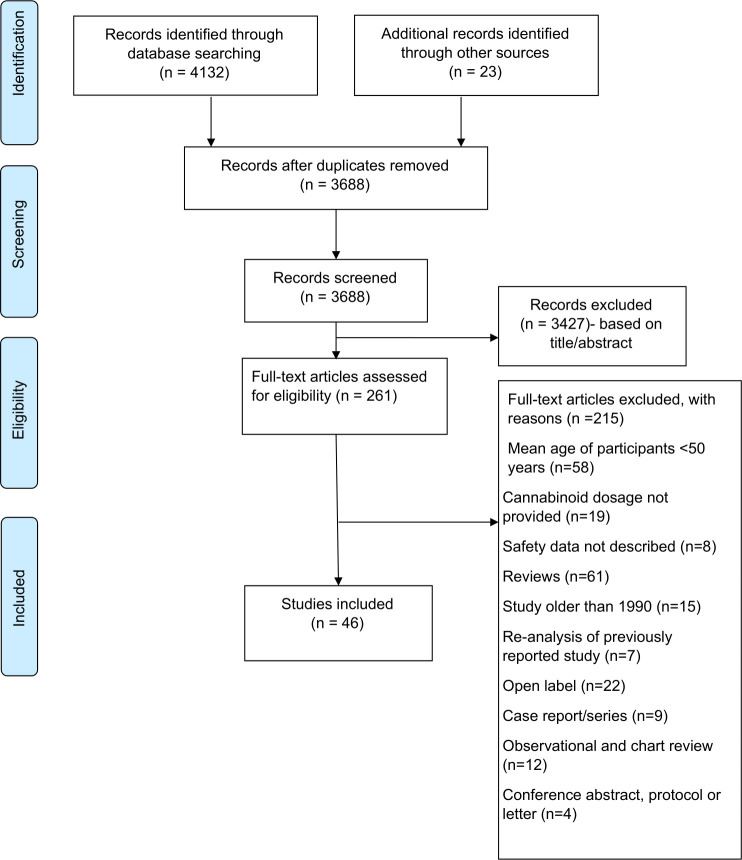
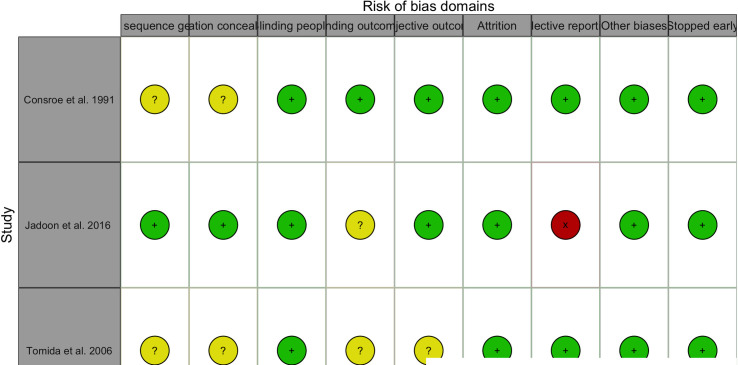
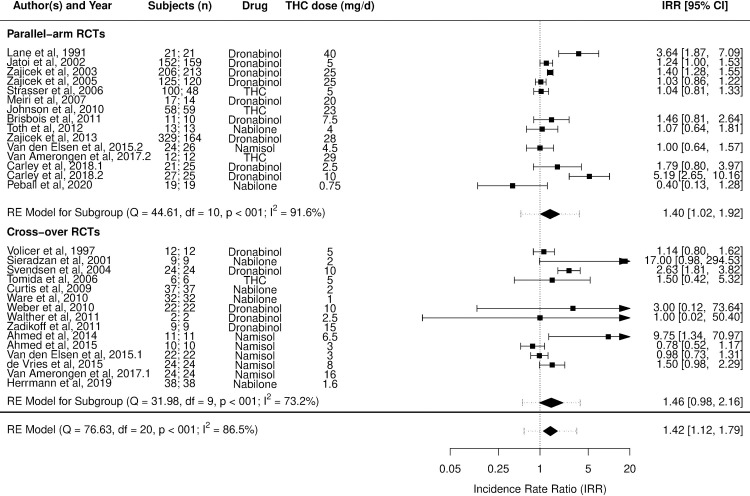
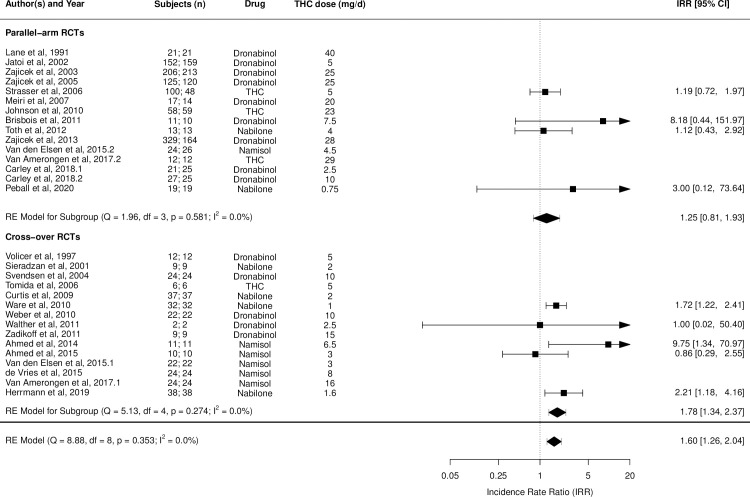
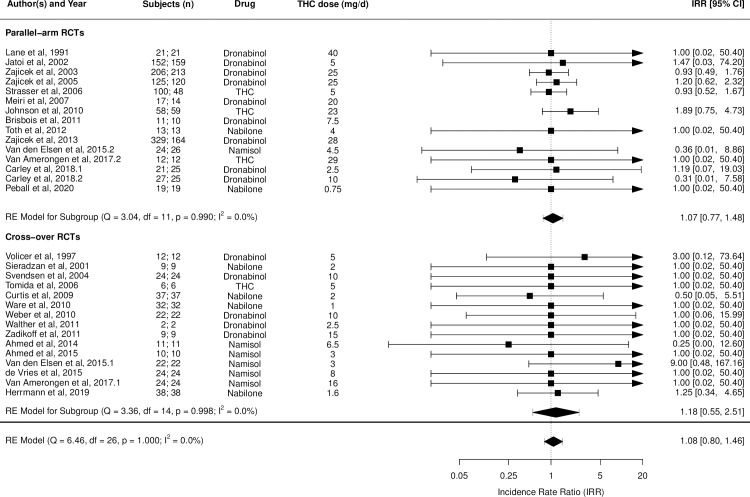
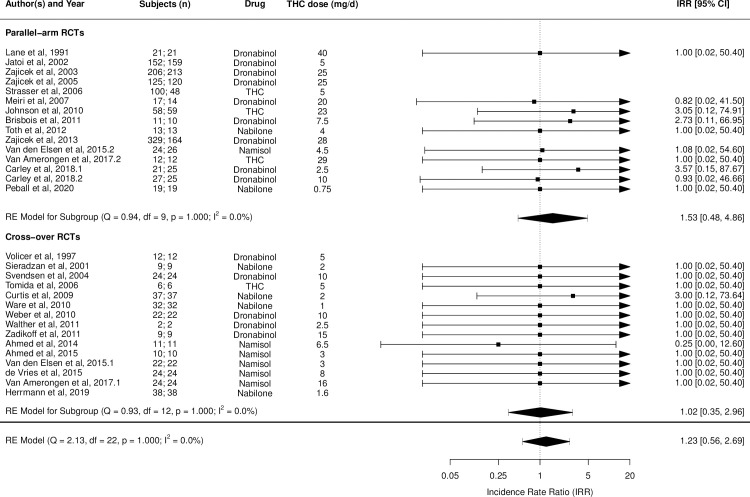
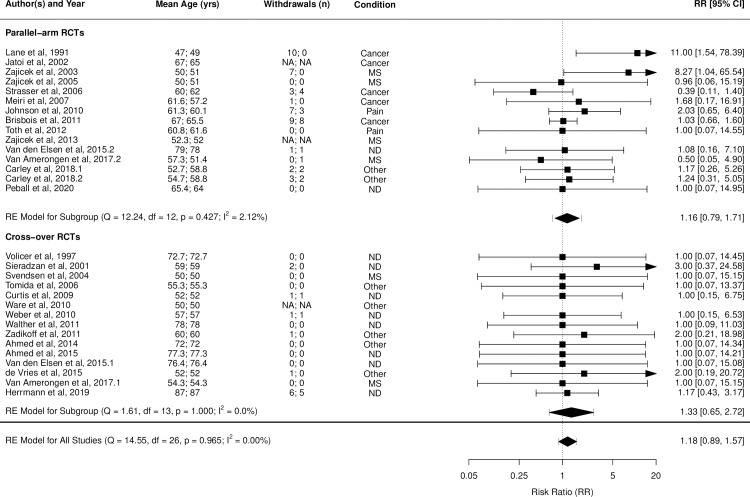
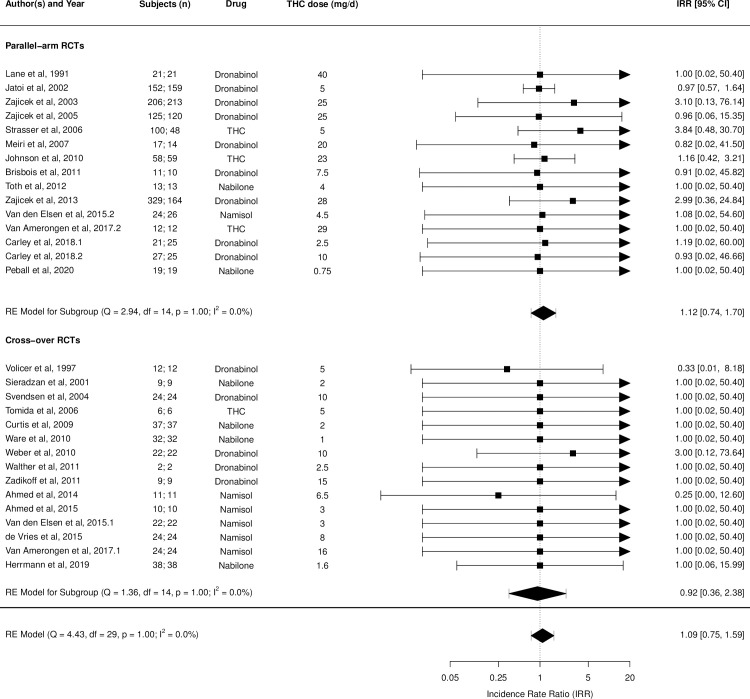
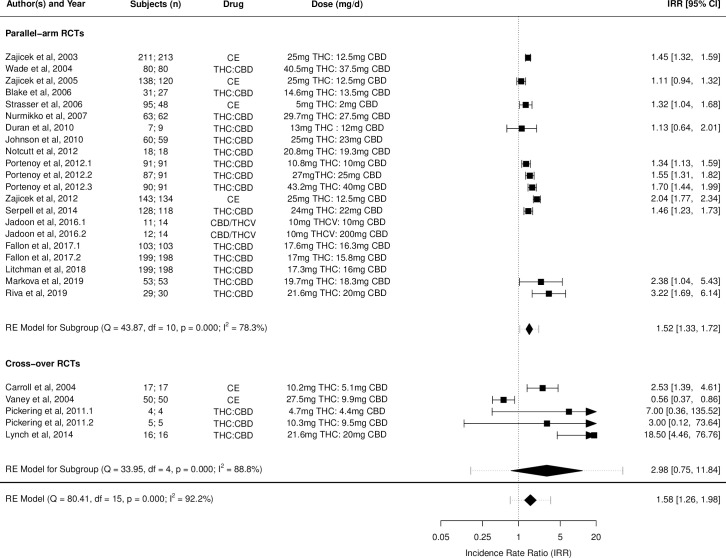
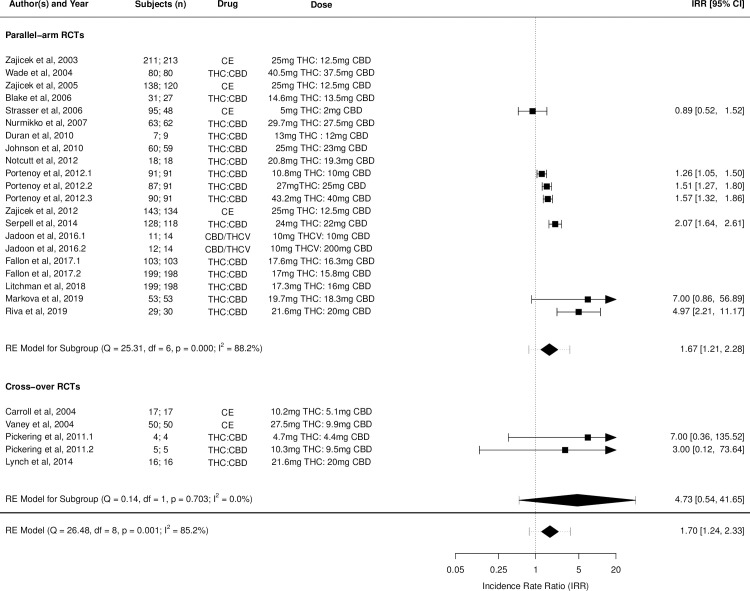
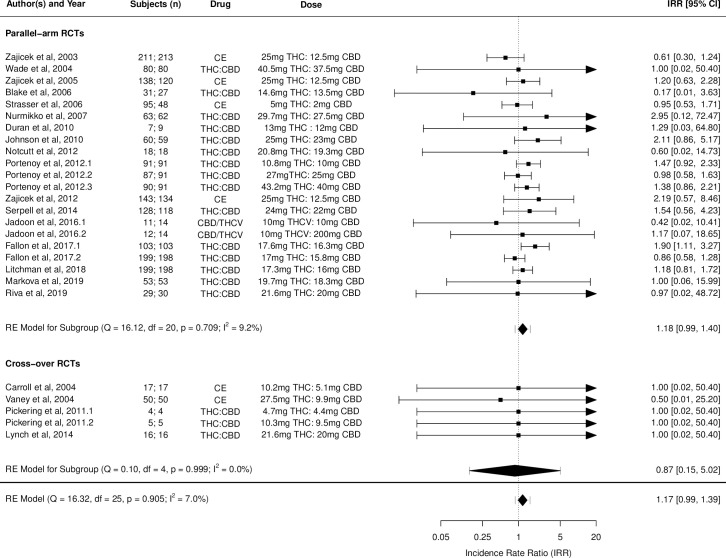
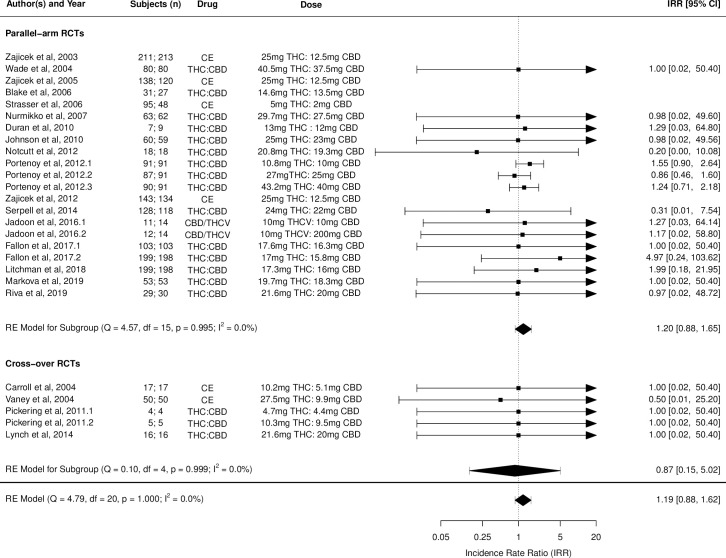
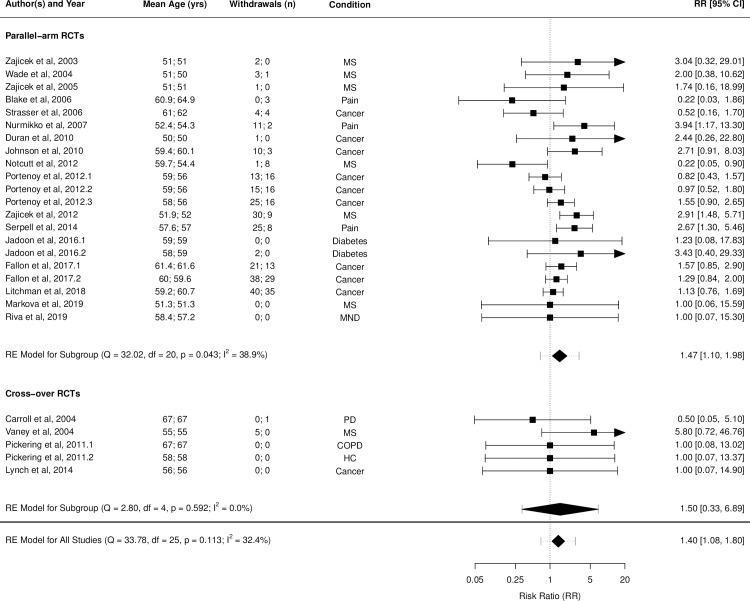
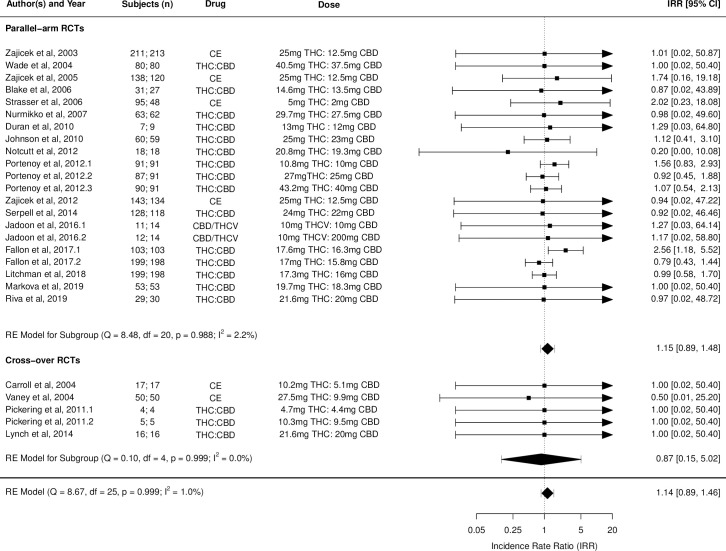
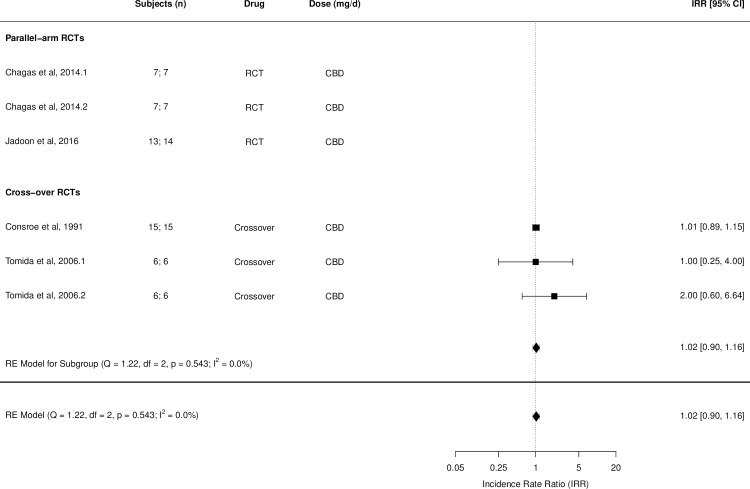
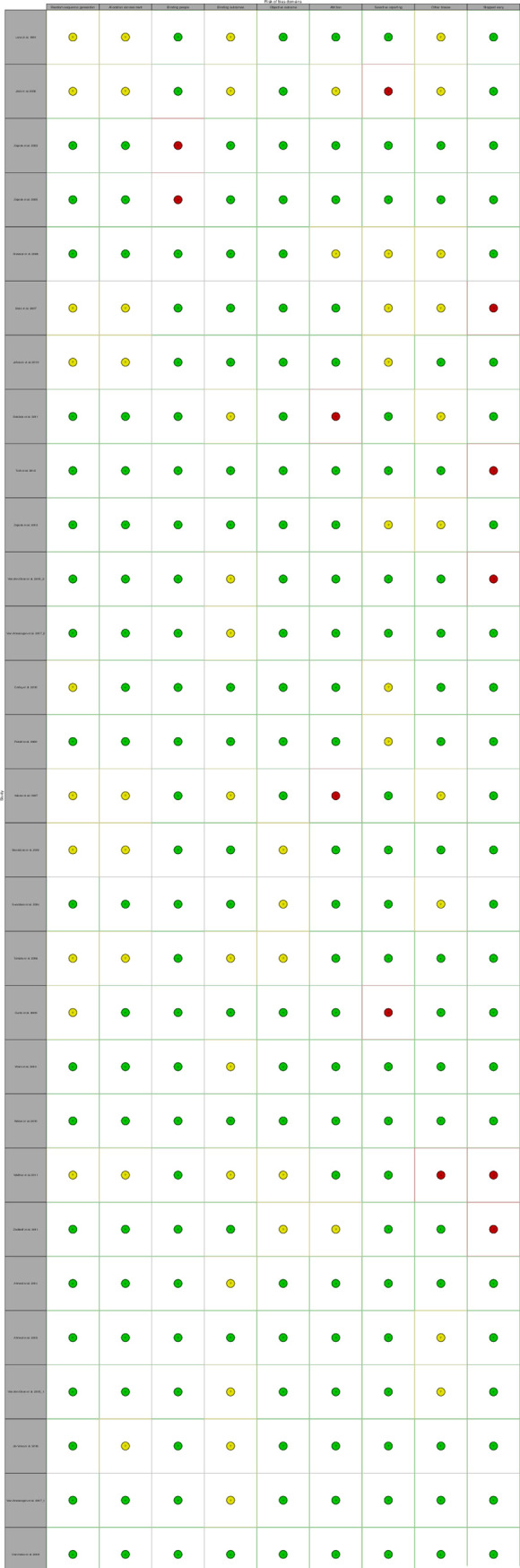
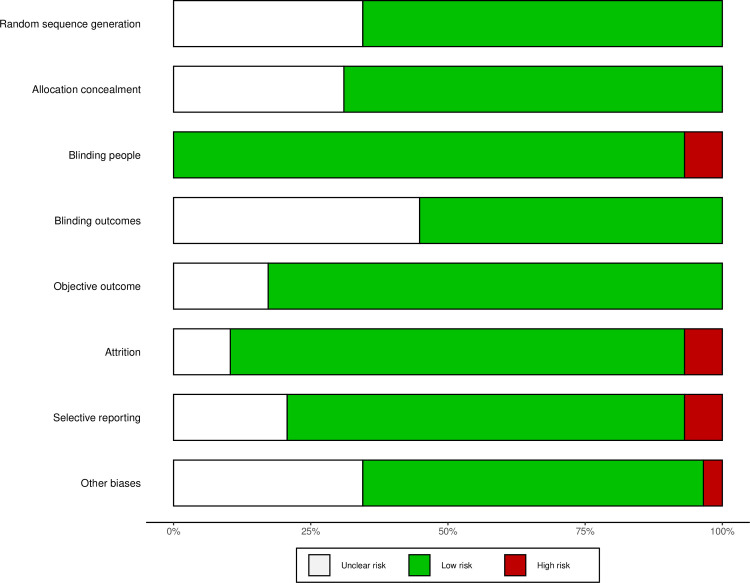
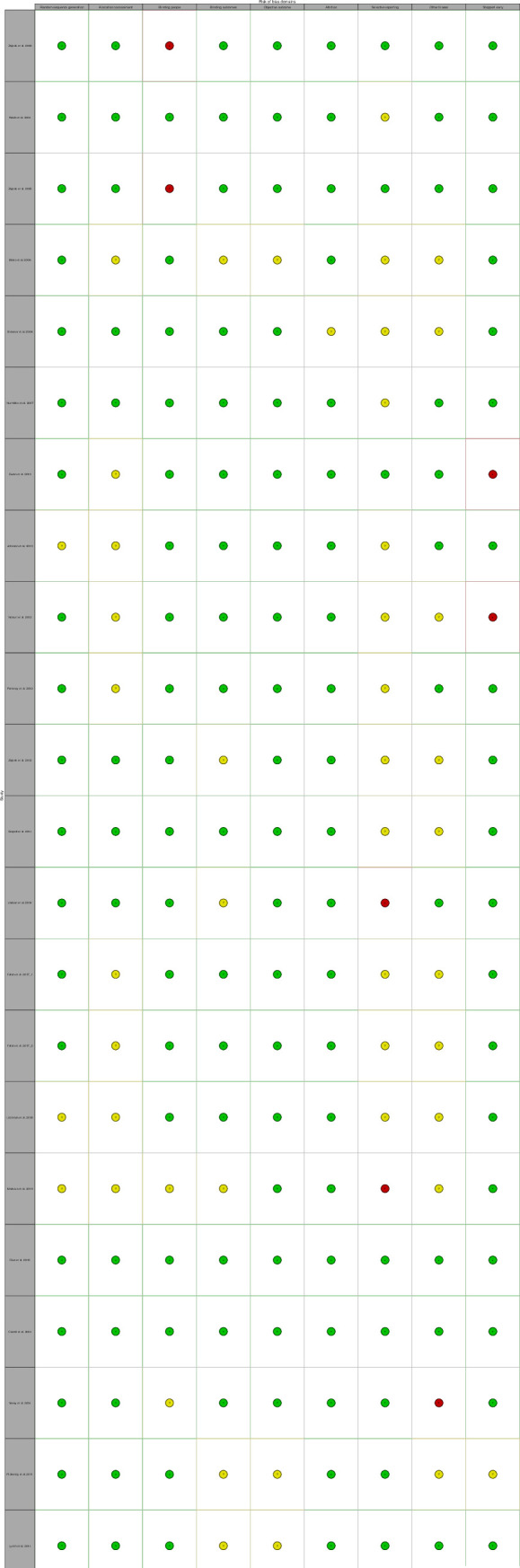
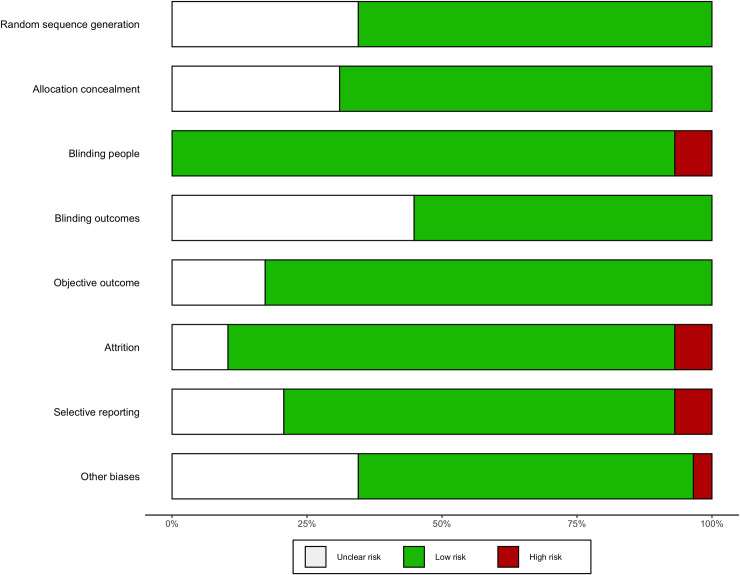
A systematic search was performed using MEDLINE, PubMed, EMBASE, CINAHL PsychInfo, Cochrane Library, and ClinicalTrials.gov (1 January 1990 to 3 October 2020). Randomised clinical trials (RCTs) of CBMs in those with mean age of ≥50 years for all indications, evaluating the safety/tolerability of CBMs where adverse events have been quantified, were included. Study quality was assessed using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) criteria and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed. Two reviewers conducted all review stages independently. Where possible, data were pooled using random-effects meta-analysis. Effect sizes were calculated as incident rate ratio (IRR) for outcome data such as adverse events (AEs), serious AEs (SAEs), and death and risk ratio (RR) for withdrawal from study and reported separately for studies using tetrahydrocannabinol (THC), THC:cannabidiol (CBD) combination, and CBD. A total of 46 RCTs were identified as suitable for inclusion of which 31 (67%) were conducted in the United Kingdom and Europe. There were 6,216 patients (mean age 58.6 ± 7.5 years; 51% male) included in the analysis, with 3,469 receiving CBMs. Compared with controls, delta-9-tetrahydrocannabinol (THC)-containing CBMs significantly increased the incidence of all-cause and treatment-related AEs: THC alone (IRR: 1.42 [95% CI, 1.12 to 1.78]) and (IRR: 1.60 [95% CI, 1.26 to 2.04]); THC:CBD combination (IRR: 1.58 [95% CI,1.26 to 1.98]) and (IRR: 1.70 [95% CI,1.24 to 2.33]), respectively. IRRs of SAEs and deaths were not significantly greater under CBMs containing THC with or without CBD. THC:CBD combination (RR: 1.40 [95% CI, 1.08 to 1.80]) but not THC alone (RR: 1.18 [95% CI, 0.89 to 1.57]) significantly increased risk of AE-related withdrawals. CBD alone did not increase the incidence of all-cause AEs (IRR: 1.02 [95% CI, 0.90 to 1.16]) or other outcomes as per qualitative synthesis. AE-related withdrawals were significantly associated with THC dose in THC only [QM (df = 1) = 4.696, p = 0.03] and THC:CBD combination treatment ([QM (df = 1) = 4.554, p = 0.033]. THC-containing CBMs significantly increased incidence of dry mouth, dizziness/light-headedness, and somnolence/drowsiness. Study limitations include inability to fully exclude data from those <50 years of age in our primary analyses as well as limitations related to weaknesses in the included trials particularly incomplete reporting of outcomes and heterogeneity in included studies.
This pooled analysis, using data from RCTs with mean participant age ≥50 years, suggests that although THC-containing CBMs are associated with side effects, CBMs in general are safe and acceptable in older adults. However, THC:CBD combinations may be less acceptable in the dose ranges used and their tolerability may be different in adults over 65 or 75 years of age.
大麻素类药物(CBMs)在老年人中广泛使用。然而,其在老年人中的安全性和耐受性尚不清楚。我们旨在对 50 岁及以上成年人使用 CBMs 的安全性和耐受性进行系统评价和荟萃分析。
使用 MEDLINE、PubMed、EMBASE、CINAHL PsychInfo、Cochrane Library 和 ClinicalTrials.gov(1990 年 1 月 1 日至 2020 年 10 月 3 日)进行系统检索。纳入了平均年龄≥50 岁的所有适应证的 CBMs 的随机对照试验(RCTs),评估了已量化不良事件的 CBMs 的安全性/耐受性。使用 GRADE(推荐评估、制定与评价)标准评估研究质量,并遵循系统评价和荟萃分析的 Preferred Reporting Items(PRISMA)指南。两名审查员独立进行了所有审查阶段。在可能的情况下,使用随机效应荟萃分析对数据进行汇总。对于不良事件(AE)、严重 AE(SAE)和退出研究等结局数据,计算发生率比(IRR)和风险比(RR),并分别报告使用四氢大麻酚(THC)、THC-大麻二酚(CBD)组合和 CBD 的研究结果。共确定了 46 项适合纳入的 RCT,其中 31 项(67%)在英国和欧洲进行。共有 6216 名患者(平均年龄 58.6±7.5 岁,51%为男性)纳入分析,其中 3469 名患者接受了 CBMs。与对照组相比,含 THC 的 CBMs 显著增加了全因和治疗相关 AE 的发生率:单独使用 THC(IRR:1.42[95%CI,1.12 至 1.78])和(IRR:1.60[95%CI,1.26 至 2.04]);THC-CBD 组合(IRR:1.58[95%CI,1.26 至 1.98])和(IRR:1.70[95%CI,1.24 至 2.33])。含 THC 或不含 CBD 的 CBMs 并不显著增加 SAE 和死亡的发生率。THC-CBD 组合(RR:1.40[95%CI,1.08 至 1.80])但单独使用 THC 不增加 AE 相关停药的风险(RR:1.18[95%CI,0.89 至 1.57])。单独使用 CBD 不增加全因 AE 的发生率(IRR:1.02[95%CI,0.90 至 1.16])或其他结局。AE 相关停药与 THC 剂量显著相关,仅含 THC 的药物[QM(df=1)=4.696,p=0.03]和 THC-CBD 组合治疗[QM(df=1)=4.554,p=0.033]。含 THC 的 CBMs 显著增加口干、头晕/头晕和嗜睡/昏睡的发生率。研究局限性包括我们的主要分析无法完全排除年龄<50 岁的数据,以及纳入试验的局限性,特别是结局报告不完整和纳入研究的异质性。
这项使用平均参与者年龄≥50 岁的 RCT 数据的汇总分析表明,尽管含 THC 的 CBMs 与副作用相关,但 CBMs 总体上在老年人中是安全和可接受的。然而,THC-CBD 组合在使用的剂量范围内可能不太容易被接受,其在 65 岁或 75 岁以上成年人中的耐受性可能不同。