Assessment and Research, American Board of Internal Medicine, Philadelphia, Pennsylvania, USA
Assessment and Research, American Board of Internal Medicine, Philadelphia, Pennsylvania, USA.
BMJ Open. 2021 Apr 1;11(4):e041817. doi: 10.1136/bmjopen-2020-041817.
Diagnostic error is a key healthcare concern and can result in substantial morbidity and mortality. Yet no study has investigated the relationship between adverse outcomes resulting from diagnostic errors and one potentially large contributor to these errors: deficiencies in diagnostic knowledge. Our objective was to measure that associations between diagnostic knowledge and adverse outcomes after visits to primary care physicians that were at risk for diagnostic errors.
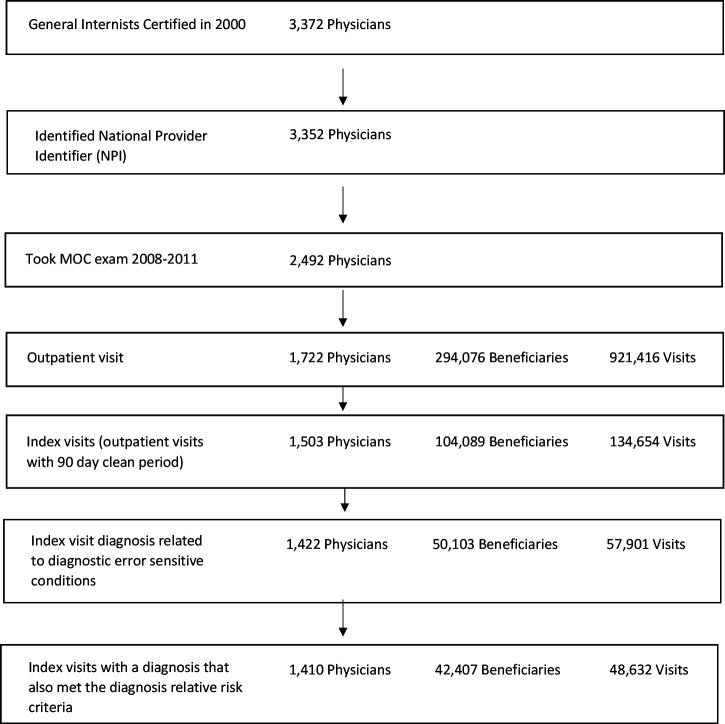
SETTING/PARTICIPANTS: 1410 US general internists who recently took their American Board of Internal Medicine Maintenance of Certification (ABIM-IM-MOC) exam treating 42 407 Medicare beneficiaries who experienced 48 632 'index' outpatient visits for new problems at risk for diagnostic error because the presenting problem (eg, dizziness) was related to prespecified diagnostic error sensitive conditions (eg, stroke).
90-day risk of all-cause death, and, for outcome conditions related to the index visits diagnosis, emergency department (ED) visits and hospitalisations.
Using retrospective cohort study design, we related physician performance on ABIM-IM-MOC diagnostic exam questions to patient outcomes during the 90-day period following an index visit at risk for diagnostic error after controlling for practice characteristics, patient sociodemographic and baseline clinical characteristics.
Rates of 90-day adverse outcomes per 1000 index visits were 7 for death, 11 for hospitalisations and 14 for ED visits. Being seen by a physician in the top versus bottom third of diagnostic knowledge during an index visit for a new problem at risk for diagnostic error was associated with 2.9 fewer all-cause deaths (95% CI -5.0 to -0.7, p=0.008), 4.1 fewer hospitalisations (95% CI -6.9 to -1.2, p=0.006) and 4.9 fewer ED visits (95% CI -8.1% to -1.6%, p=0.003) per 1000 visits.
Higher diagnostic knowledge was associated with lower risk of adverse outcomes after visits for problems at heightened risk for diagnostic error.
诊断错误是一个关键的医疗保健问题,可能导致大量的发病率和死亡率。然而,尚无研究调查导致诊断错误的不良后果与这些错误的一个潜在大贡献者之间的关系:诊断知识的缺陷。我们的目的是衡量在初级保健医生就诊期间,诊断知识与因诊断错误风险较高的新问题就诊后不良后果之间的关联。
背景/参与者:1410 名美国普通内科医生最近参加了他们的美国内科医师学会内科医学维护认证(ABIM-IM-MOC)考试,治疗了 42407 名 Medicare 受益人,他们经历了 48632 次新问题的“索引”门诊就诊,这些问题存在诊断错误的风险,因为就诊问题(例如,头晕)与预定的诊断错误敏感条件(例如,中风)有关。
90 天全因死亡率,以及与索引就诊诊断相关的结局情况,包括急诊科就诊和住院治疗。
使用回顾性队列研究设计,我们将医生在 ABIM-IM-MOC 诊断考试问题上的表现与 90 天内索引就诊后患者的结局相关联,这些索引就诊存在诊断错误的风险,在控制了实践特征、患者社会人口统计学和基线临床特征后。
每 1000 次索引就诊的 90 天不良结局发生率为死亡 7 例,住院 11 例,急诊科就诊 14 例。在新问题的索引就诊期间,与诊断错误风险较高的问题就诊时,医生的诊断知识处于前三分位与后三分位之间,与全因死亡减少 2.9 例(95%CI-5.0 至-0.7,p=0.008)、住院治疗减少 4.1 例(95%CI-6.9 至-1.2,p=0.006)和急诊科就诊减少 4.9 例(95%CI-8.1%至-1.6%,p=0.003)相关。
较高的诊断知识与因诊断错误风险较高的问题就诊后不良后果风险较低相关。