Pfaar Oliver, Klimek Ludger, Hamelmann Eckard, Kleine-Tebbe Jörg, Taube Christian, Wagenmann Martin, Werfel Thomas, Brehler Randolf, Novak Natalija, Mülleneisen Norbert, Becker Sven, Worm Margitta
Department of Otorhinolaryngology, Head and Neck Surgery, Section of Rhinology and Allergy, University Hospital Marburg, Philipps-Universität Marburg.
Center for Rhinology and Allergology, Wiesbaden.
Allergol Select. 2021 Apr 1;5:140-147. doi: 10.5414/ALX02241E. eCollection 2021.
After the beginning and during the worldwide pandemic caused by the severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2), patients with allergic and atopic diseases have felt and still feel insecure. Currently, four vaccines against SARS-CoV-2 have been approved by the Paul Ehrlich Institute in Germany, and vaccination campaigns have been started nationwide. In this respect, it is of utmost importance to give recommendations on possible immunological interactions and potential risks of immunomodulatory substances (monoclonal antibodies, biologicals) during concurrent vaccination with the approved vaccines.
This position paper provides specific recommendations on the use of immunomodulatory drugs in the context of concurrent SARS-CoV-2 vaccinations based on current literature.
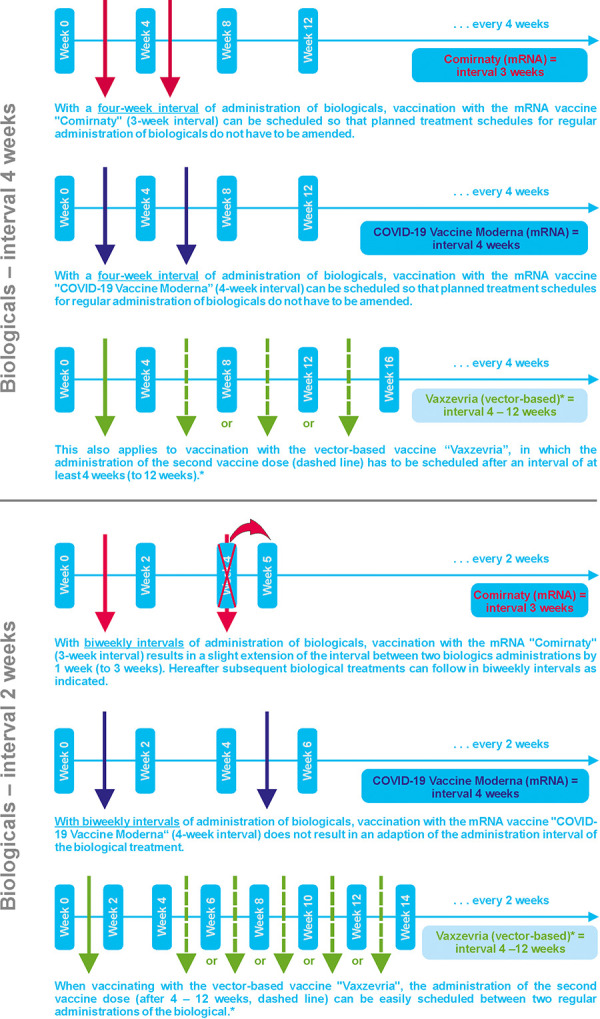
The recommendations are covering the following conditions in which biologicals are indicated and approved: 1) chronic inflammatory skin diseases (atopic dermatitis, chronic spontaneous urticaria), 2) bronchial asthma, and 3) chronic rhinosinusitis with nasal polyps (CRSwNP). Patients with atopic dermatitis or chronic spontaneous urticaria are not at increased risk for allergic reactions after COVID-19 vaccination. Nevertheless, vaccination may result in transient eczema exacerbation due to general immune stimulation. Vaccination in patients receiving systemic therapy with biologicals can be performed. Patients with severe asthma and concomitant treatment with biologicals also do not have an increased risk of allergic reaction following COVID-19 vaccination which is recommended in these patients. Patients with CRSwNP are also not known to be at increased risk for allergic vaccine reactions, and continuation or initiation of a treatment with biologicals is also recommended with concurrent COVID-19 vaccination. In general, COVID-19 vaccination should be given within the interval between two applications of the respective biological, that is, with a time-lag of at least 1 week after the previous or at least 1 week before the next biological treatment planned.
Biologicals for the treatment of atopic dermatitis, chronic spontaneous urticaria, bronchial asthma, and CRSwNP should be continued during the current COVID-19 vaccination campaigns. However, the intervals of biological treatment may need to be slightly adjusted (DGAKI/AeDA recommendations as of March 22, 2021).
在严重急性呼吸综合征冠状病毒2型(SARS-CoV-2)引发的全球大流行开始后及流行期间,患有过敏性和特应性疾病的患者一直并仍感到不安。目前,德国保罗·埃利希研究所已批准四种针对SARS-CoV-2的疫苗,全国范围内已启动疫苗接种活动。在这方面,就同时接种已批准疫苗期间免疫调节物质(单克隆抗体、生物制剂)可能的免疫相互作用和潜在风险给出建议至关重要。
本立场文件基于当前文献,就同时接种SARS-CoV-2疫苗的情况下免疫调节药物的使用提供具体建议。
建议涵盖以下使用生物制剂且已获批准的情况:1)慢性炎症性皮肤病(特应性皮炎、慢性自发性荨麻疹),2)支气管哮喘,3)伴有鼻息肉的慢性鼻-鼻窦炎(CRSwNP)。患有特应性皮炎或慢性自发性荨麻疹的患者在接种新冠疫苗后发生过敏反应的风险并未增加。然而,由于全身免疫刺激,接种疫苗可能导致湿疹短暂加重。接受生物制剂全身治疗的患者可以接种疫苗。患有严重哮喘且接受生物制剂治疗的患者在接种新冠疫苗后发生过敏反应的风险也未增加,这些患者建议接种疫苗。CRSwNP患者接种疫苗后发生过敏反应的风险也未增加,同时接种新冠疫苗时也建议继续或开始生物制剂治疗。一般而言,新冠疫苗接种应在各自生物制剂两次用药的间隔期内进行,即在之前一次生物制剂治疗后至少间隔1周或在下一次计划的生物制剂治疗前至少间隔1周。
在当前的新冠疫苗接种活动期间,用于治疗特应性皮炎、慢性自发性荨麻疹、支气管哮喘和CRSwNP的生物制剂应继续使用。然而,生物制剂治疗的间隔时间可能需要稍作调整(截至2021年3月22日的德国变态反应和临床免疫学会/德国皮肤病学会建议)。