Department of Population Health Sciences, Weill Cornell Medicine, New York, NY, United States.
Joan and Sanford I. Weill Department of Medicine, Weill Cornell Medicine, New York, NY, United States.
J Biomed Inform. 2021 Jun;118:103794. doi: 10.1016/j.jbi.2021.103794. Epub 2021 Apr 30.
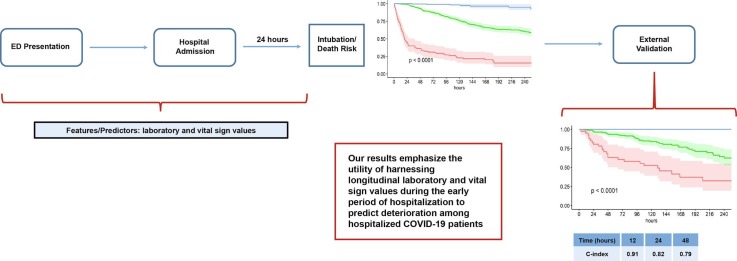
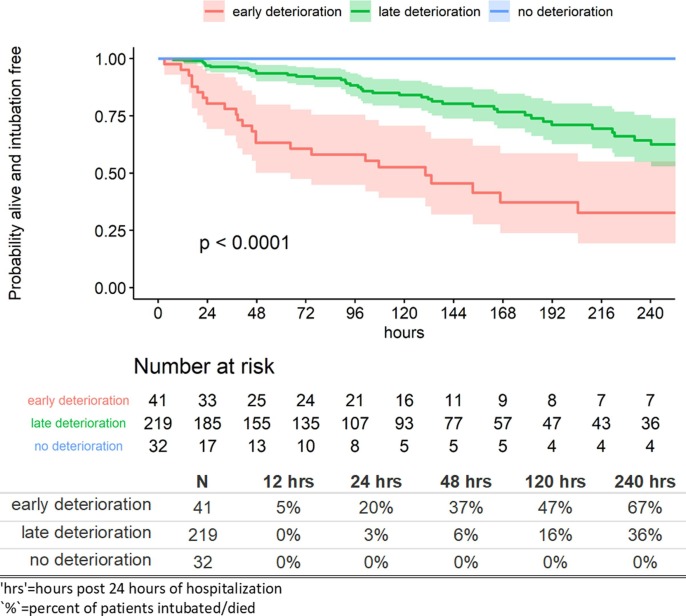
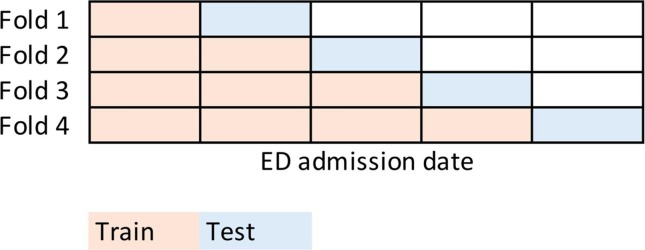
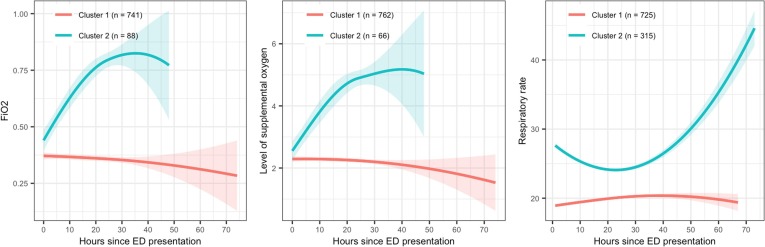
From early March through mid-May 2020, the COVID-19 pandemic overwhelmed hospitals in New York City. In anticipation of ventilator shortages and limited ICU bed capacity, hospital operations prioritized the development of prognostic tools to predict clinical deterioration. However, early experience from frontline physicians observed that some patients developed unanticipated deterioration after having relatively stable periods, attesting to the uncertainty of clinical trajectories among hospitalized patients with COVID-19. Prediction tools that incorporate clinical variables at one time-point, usually on hospital presentation, are suboptimal for patients with dynamic changes and evolving clinical trajectories. Therefore, our study team developed a machine-learning algorithm to predict clinical deterioration among hospitalized COVID-19 patients by extracting clinically meaningful features from complex longitudinal laboratory and vital sign values during the early period of hospitalization with an emphasis on informative missing-ness. To incorporate the evolution of the disease and clinical practice over the course of the pandemic, we utilized a time-dependent cross-validation strategy for model development. Finally, we validated our prediction model on an external validation cohort of COVID-19 patients served in a demographically distinct population from the training cohort. The main finding of our study is the identification of risk profiles of early, late and no clinical deterioration during the course of hospitalization. While risk prediction models that include simple predictors at ED presentation and clinical judgement are able to identify any deterioration vs. no deterioration, our methodology is able to isolate a particular risk group that remain stable initially but deteriorate at a later stage of the course of hospitalization. We demonstrate the superior predictive performance with the utilization of laboratory and vital sign data during the early period of hospitalization compared to the utilization of data at presentation alone. Our results will allow efficient hospital resource allocation and will motivate research in understanding the late deterioration risk group.
从 2020 年 3 月初到 5 月中旬,COVID-19 疫情使纽约市的医院不堪重负。为了应对呼吸机短缺和 ICU 床位容量有限的问题,医院运营部门优先开发了预测工具,以预测临床恶化的情况。然而,一线医生的早期经验观察到,一些患者在相对稳定的时期后出现了意料之外的恶化,这证明了 COVID-19 住院患者的临床轨迹存在不确定性。仅在住院时的一个时间点(通常在就诊时)纳入临床变量的预测工具,对于具有动态变化和不断发展的临床轨迹的患者来说并不理想。因此,我们的研究团队开发了一种机器学习算法,通过从住院期间复杂的纵向实验室和生命体征值中提取有意义的特征,来预测 COVID-19 住院患者的临床恶化情况,重点关注有意义的缺失值。为了纳入疾病和临床实践在疫情期间的演变,我们利用了一种时间相关的交叉验证策略来开发模型。最后,我们在一个与训练队列人口统计学不同的 COVID-19 患者外部验证队列上验证了我们的预测模型。我们研究的主要发现是确定了住院期间早期、晚期和无临床恶化的风险特征。虽然包括 ED 就诊时简单预测因子和临床判断的风险预测模型能够识别任何恶化与无恶化,但我们的方法能够分离出一个最初稳定但在住院过程后期恶化的特定风险组。与仅在就诊时使用数据相比,我们通过在住院早期使用实验室和生命体征数据,证明了优越的预测性能。我们的研究结果将有助于实现有效的医院资源分配,并激发对理解晚期恶化风险组的研究。