Marsman Martijn S, Wetterslev Jørn, Jahrome Abdelkarime Kh, Gluud Christian, Moll Frans L, Keus Frederik, Koning Giel G
Department of Vascular Surgery, Rijnstate Hospital, Wagnerlaan 55, 6815 AD, Arnhem, the Netherlands.
Copenhagen Trial Unit, Centre for Clinical Intervention Research, The Capital Region of Denmark, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark.
Syst Rev. 2021 May 6;10(1):139. doi: 10.1186/s13643-021-01692-8.
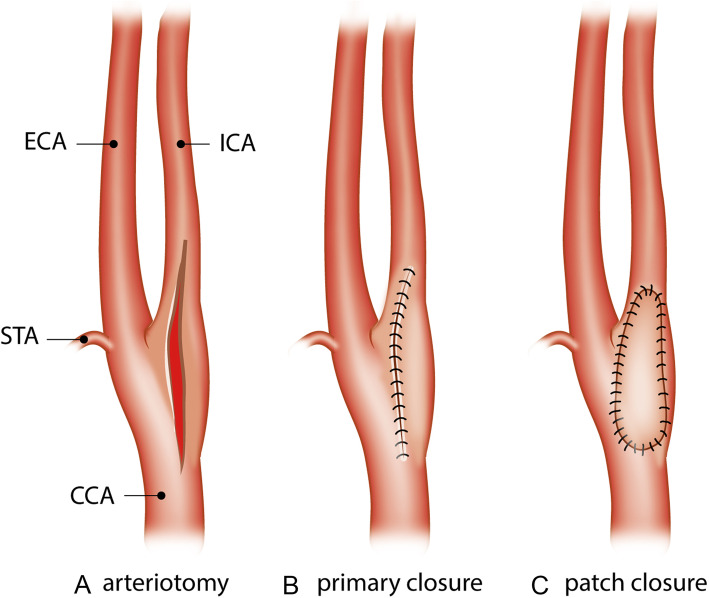
Patch angioplasty in conventional carotid endarterectomy is suggested to reduce the risk of restenosis and recurrent ipsilateral stroke compared with primary closure. A systematic review of randomized clinical trials is needed to compare outcomes (benefits and harms) of both techniques.
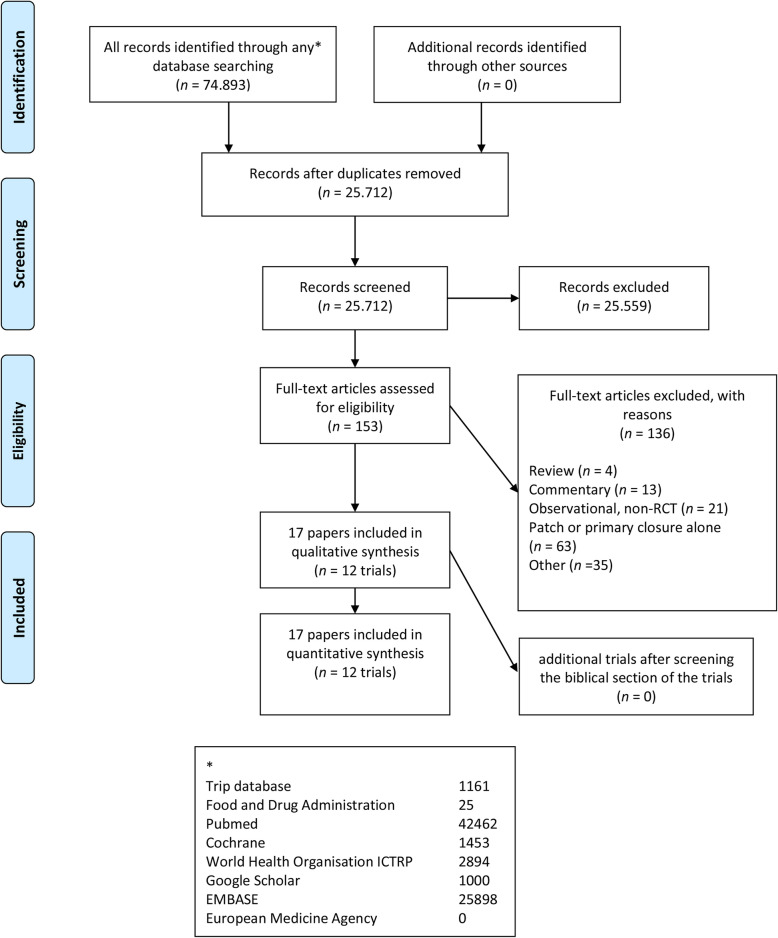
Searches (CENTRAL, PubMed/MEDLINE, EMBASE, and other databases) were last updated 3rd of January 2021. We included randomized clinical trials comparing carotid endarterectomy with patch angioplasty versus primary closure of the arterial wall in patients with a symptomatic and significant (> 50%) carotid stenosis. Primary outcomes are defined as all-cause mortality and serious adverse events.
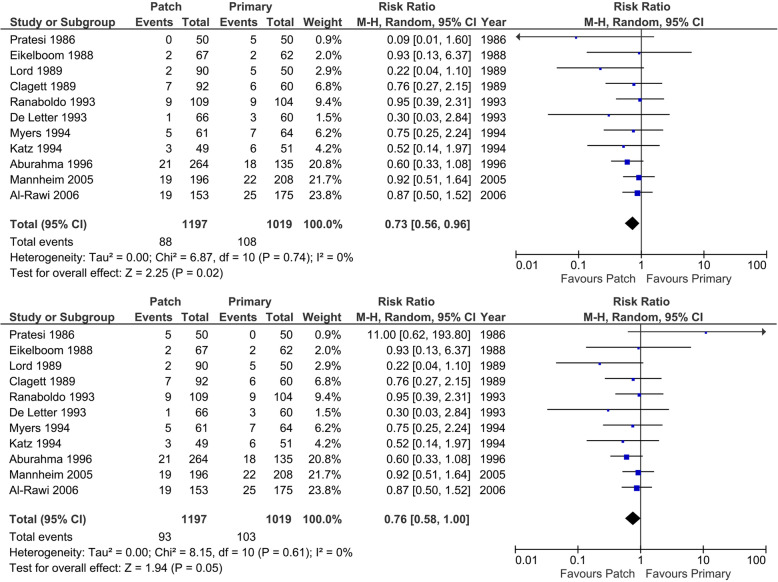
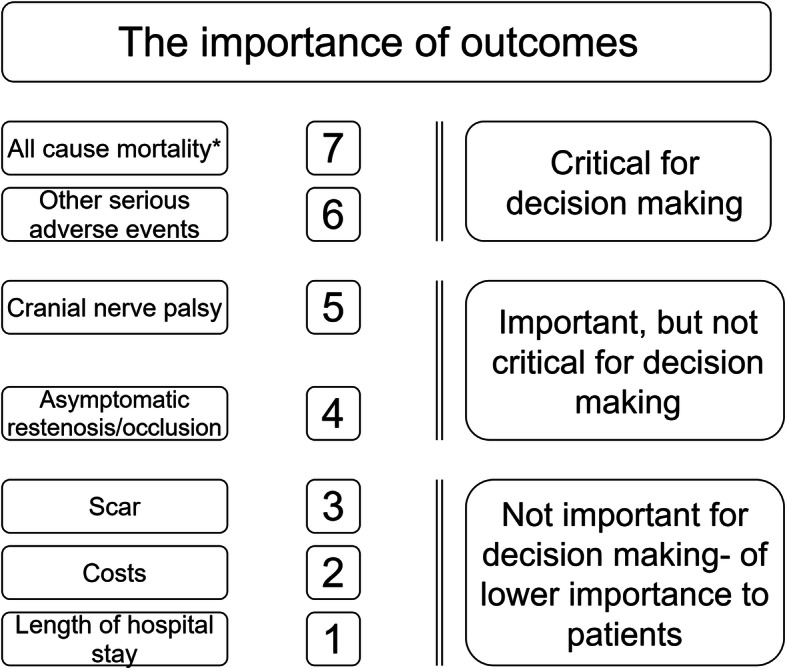
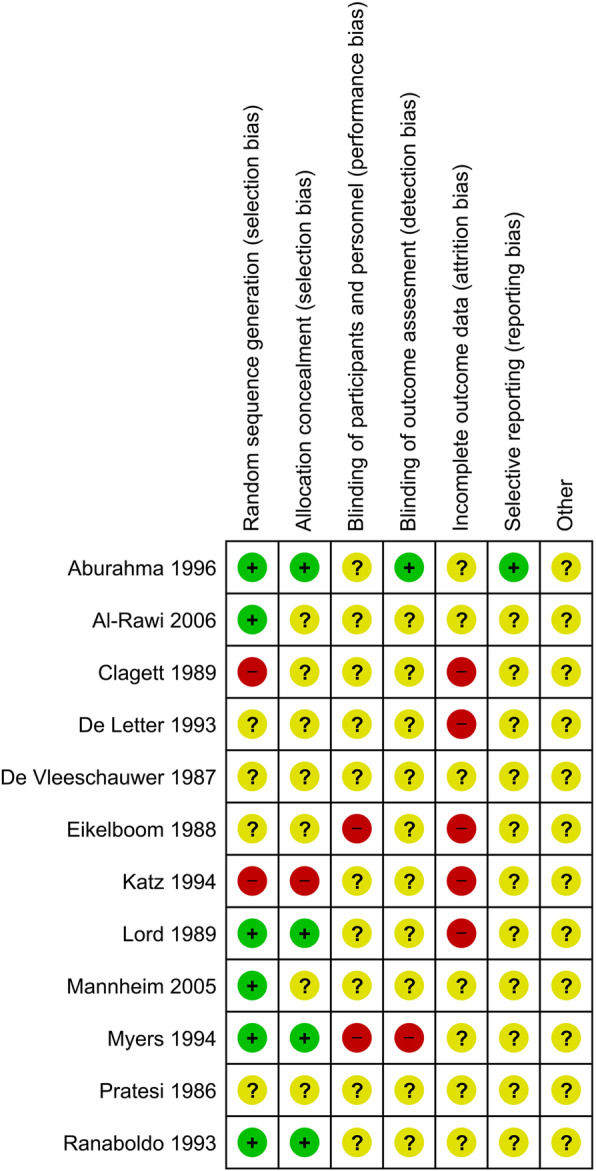
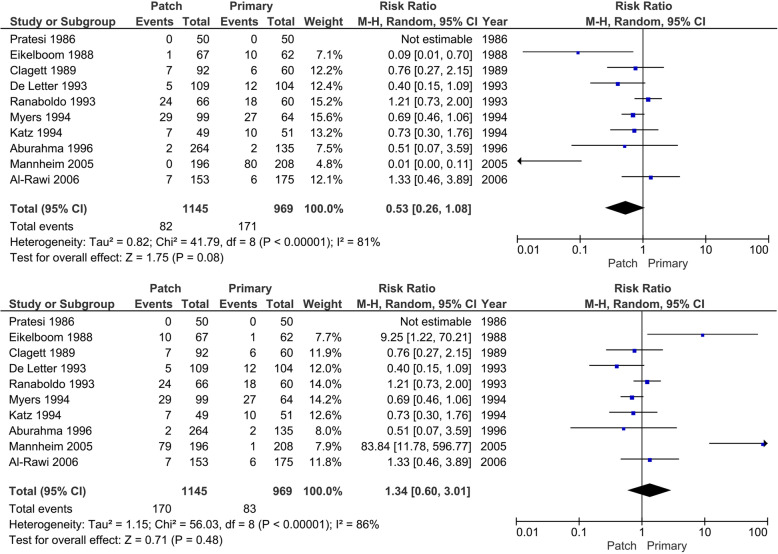
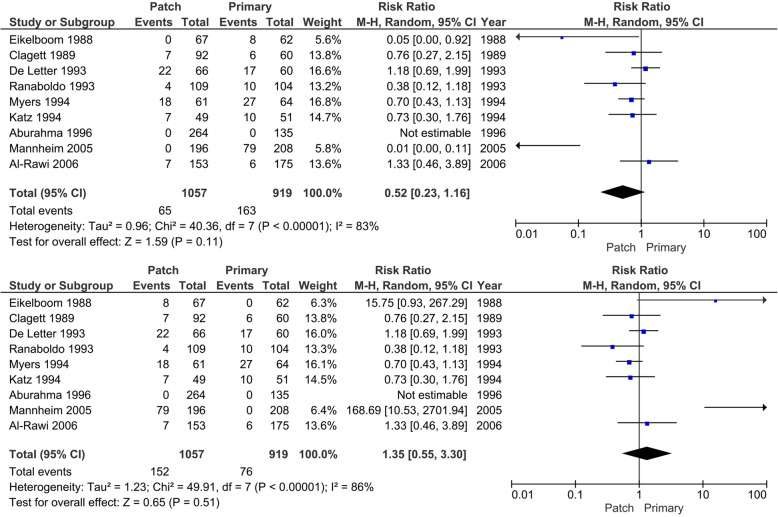
We included 12 randomized clinical trials including 2187 participants who underwent 2335 operations for carotid stenosis comparing carotid endarterectomy with patch closure (1280 operations) versus carotid endarterectomy with primary closure (1055 operations). Meta-analysis comparing carotid endarterectomy with patch angioplasty versus carotid endarterectomy with primary closure may potentially decrease the number of patients with all-cause mortality (RR 0.53; 95% CI 0.26 to 1.08; p = 0.08, best-case scenario for patch), serious adverse events (RR 0.73; 95% CI 0.56 to 0.96; p = 0.02, best-case scenario for patch), and the number of restenosis (RR 0.41; 95% CI 0.23 to 0.71; p < 0.01). Trial sequential analysis demonstrated that the required information sizes were far from being reached for these patient-important outcomes. All the patient-relevant outcomes were at low certainty of evidence according to The Grading of Recommendations Assessment, Development, and Evaluation.
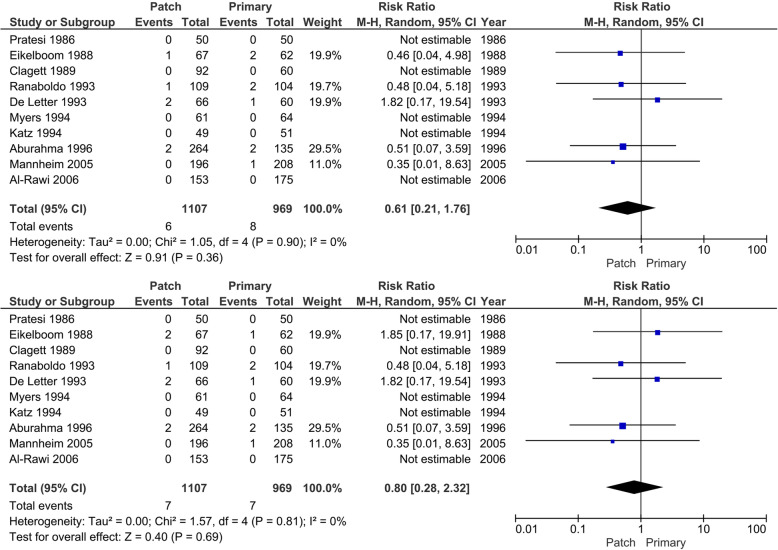
This systematic review showed no conclusive evidence of a difference between carotid endarterectomy with patch angioplasty versus primary closure of the arterial wall on all-cause mortality, < 30 days mortality, < 30 days stroke, or any other serious adverse events. These conclusions are based on data from 15 to 35 years ago, obtained in trials with very low certainty according to GRADE, and should be interpreted cautiously. Therefore, we suggest conducting new randomized clinical trials patch angioplasty versus primary closure in carotid endarterectomy in symptomatic patients with an internal carotid artery stenosis of 50% or more. Such trials ought to be designed according to the Standard Protocol Items: Recommendations for Interventional Trials statement (Chan et al., Ann Intern Med 1:200-7, 2013) and reported according to the Consolidated Standards of Reporting Trials statement (Schulz et al., 7, 2010). Until conclusive evidence is obtained, the standard of care according to guidelines should not be abandoned.
PROSPERO CRD42014013416 . Review protocol publication 2019 DOI: https://doi.org/10.1136/bmjopen-2018-026419 .
与直接缝合相比,传统颈动脉内膜切除术采用补片血管成形术可降低再狭窄和同侧复发性卒中的风险。需要对随机临床试验进行系统评价,以比较两种技术的疗效(益处和危害)。
检索(CENTRAL、PubMed/MEDLINE、EMBASE及其他数据库)于2021年1月3日最后更新。我们纳入了比较有症状且严重(>50%)颈动脉狭窄患者行颈动脉内膜切除术加补片血管成形术与动脉壁直接缝合的随机临床试验。主要结局定义为全因死亡率和严重不良事件。
我们纳入了12项随机临床试验,共2187名参与者接受了2335例颈动脉狭窄手术,比较颈动脉内膜切除术加补片缝合(1280例手术)与颈动脉内膜切除术直接缝合(1055例手术)。对颈动脉内膜切除术加补片血管成形术与颈动脉内膜切除术直接缝合进行的荟萃分析可能会降低全因死亡患者数量(风险比0.53;95%置信区间0.26至1.08;p = 0.08,补片的最佳情况)、严重不良事件(风险比0.73;95%置信区间0.56至0.96;p = 0.02,补片的最佳情况)以及再狭窄数量(风险比0.41;95%置信区间0.23至0.71;p < 0.01)。试验序贯分析表明,对于这些对患者重要的结局,所需的信息量远未达到。根据推荐分级评估、制定和评价,所有与患者相关的结局证据确定性均较低。
本系统评价未发现确凿证据表明颈动脉内膜切除术加补片血管成形术与动脉壁直接缝合在全因死亡率、<30天死亡率、<30天卒中或任何其他严重不良事件方面存在差异。这些结论基于15至35年前的数据,这些数据来自根据GRADE确定性非常低的试验,应谨慎解读。因此,我们建议对有症状的颈内动脉狭窄50%或以上的患者,在颈动脉内膜切除术中进行补片血管成形术与直接缝合的新随机临床试验。此类试验应根据《干预试验标准方案条目:建议》声明(Chan等人,《内科学年鉴》1:200 - 7,2013年)进行设计,并根据《试验报告统一标准》声明(Schulz等人,2010年,7)进行报告。在获得确凿证据之前,不应放弃指南规定的治疗标准。
PROSPERO CRD42014013416 。评价方案发表于2019年,DOI: https://doi.org/10.1136/bmjopen - 2018 - 026419 。