Midena Edoardo, Torresin Tommaso, Velotta Erika, Pilotto Elisabetta, Parrozzani Raffaele, Frizziero Luisa
Department of Ophthalmology, University of Padova, Padova, Italy.
IRCCS-Fondazione Bietti, Rome, Italy.
Front Immunol. 2021 Apr 22;12:613051. doi: 10.3389/fimmu.2021.613051. eCollection 2021.
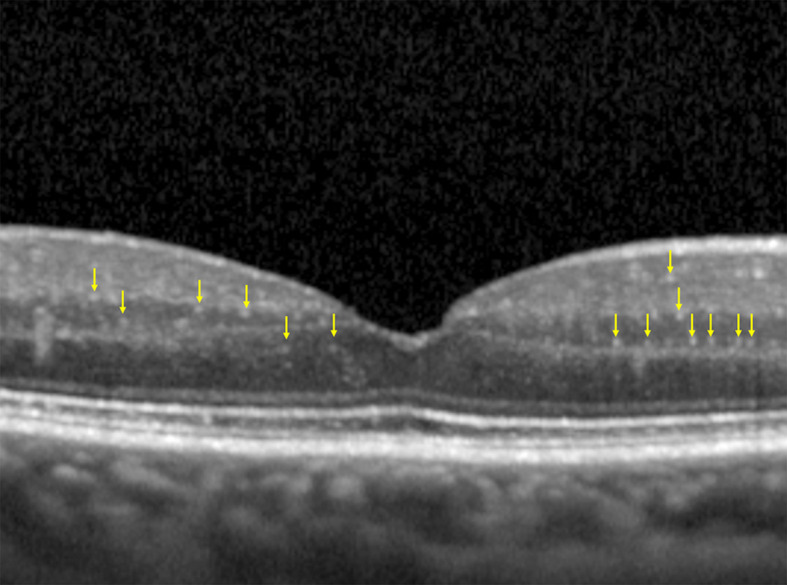
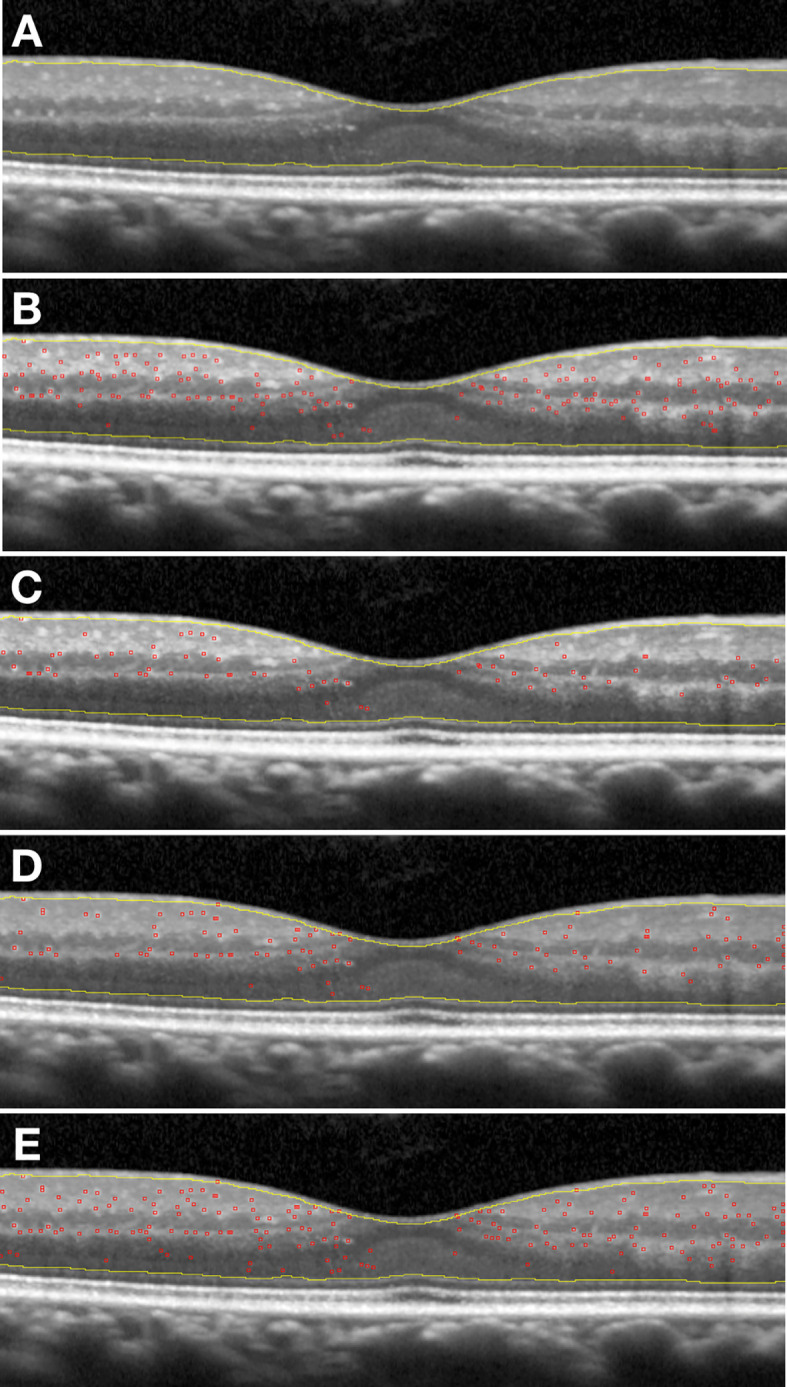
Optical coherence tomography (OCT) allows us to identify, into retinal layers, new morphological entities, which can be considered clinical biomarkers of retinal diseases. According to the literature, solitary, small (<30 µm), medium level hyperreflective (similar to retinal fiber layer) retinal foci (HRF) may represent aggregates of activated microglial cells and an biomarker of retinal inflammation. The identification and quantification of this imaging biomarker allows for estimating the level and possibly the amount of intraretinal inflammation in major degenerative retinal disorders, whose inflammatory component has already been demonstrated (diabetic retinopathy, age-related macular degeneration, radiation retinopathy). Currently, diabetic retinopathy (DR) probably represents the best clinical model to apply this analysis in the definition of this clinical biomarker. However, the main limitation to the clinical use of HRF is related to the technical difficulty of counting them: a time-consuming methodology, which also needs trained examiners. To contribute to solve this limitation, we developed and validated a new method for the semi-automatic detection of HRF in OCT scans. OCT scans of patients affected by DR, were analyzed. HRF were manually counted in High Resolution spectral domain OCT images. Then, the same OCT scans underwent semi-automatic HRF counting, using an ImageJ software with four different settings profiles. Statistical analysis showed an excellent intraclass correlation coefficient (ICC) between the manual count and each of the four semi-automated methods. The use of the second setting profile allows to obtain at the Bland-Altman graph a of -0.2 foci and a limit of agreement of ±16.3 foci. This validation approach opens the way not only to the reliable and daily clinical applicable quantification of HRF, but also to a better knowledge of the inflammatory component-including its progression and regression changes-of diabetic retinopathy.
光学相干断层扫描(OCT)使我们能够在视网膜各层中识别出新的形态学实体,这些实体可被视为视网膜疾病的临床生物标志物。根据文献,孤立的、小的(<30 µm)、中等水平高反射性(类似于视网膜纤维层)的视网膜病灶(HRF)可能代表活化小胶质细胞的聚集体,是视网膜炎症的生物标志物。对这种成像生物标志物的识别和定量有助于估计主要退行性视网膜疾病中视网膜内炎症的水平以及可能的炎症量,这些疾病的炎症成分已得到证实(糖尿病性视网膜病变、年龄相关性黄斑变性、放射性视网膜病变)。目前,糖尿病性视网膜病变(DR)可能是应用这种分析来定义这种临床生物标志物的最佳临床模型。然而,HRF临床应用的主要限制与计数的技术难度有关:这是一种耗时的方法,还需要训练有素的检查人员。为了有助于解决这一限制,我们开发并验证了一种在OCT扫描中半自动检测HRF的新方法。对患有DR的患者的OCT扫描进行了分析。在高分辨率光谱域OCT图像中手动计数HRF。然后,使用具有四种不同设置配置文件的ImageJ软件对相同的OCT扫描进行半自动HRF计数。统计分析显示手动计数与四种半自动方法中的每一种之间都有出色的组内相关系数(ICC)。使用第二种设置配置文件在布兰德-奥特曼图上可得到-0.2个病灶的偏差和±16.3个病灶的一致性界限。这种验证方法不仅为HRF的可靠且日常临床适用的定量分析开辟了道路,也为更好地了解糖尿病性视网膜病变的炎症成分(包括其进展和消退变化)开辟了道路。