Laghlam Driss, Naudin Cecile, Coroyer Lucas, Aidan Vincent, Malvy Julien, Rahoual Ghilas, Estagnasié Philippe, Squara Pierre
Department of Cardiology and Critical Care, CERIC, Clinique Ambroise Paré, 27 boulevard Victor Hugo, 92200, Neuilly-sur-Seine, France.
Department of Clinical Research, Clinique Ambroise Paré, 27 boulevard Victor Hugo, 92200, Neuilly-sur-Seine, France.
Ann Intensive Care. 2021 May 13;11(1):74. doi: 10.1186/s13613-021-00866-w.
The management of pain and anxiety remains a challenge in the intensive care unit. By distracting patients, virtual reality (VR) may have a role in painful procedures. We compared VR vs. an inhaled equimolar mixture of NO and O (Kalinox®) for pain and anxiety management during the removal of chest drains after cardiac surgery.
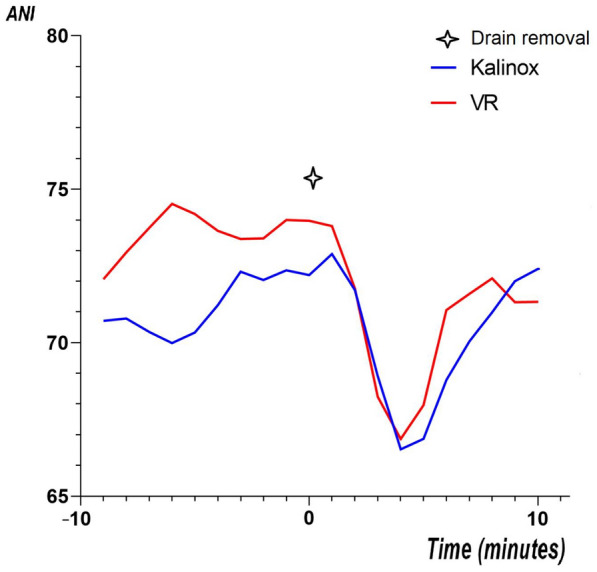
Prospective, non-inferiority, open-label study. Patients were randomized, for Kalinox® or VR session during drain removal. The analgesia/nociception index (ANI) was monitored during the procedure for objective assessment of pain and anxiety. The primary endpoint was the ΔANI (ANI - ANI) during the procedure, based on ANIm (average on 4 min). We prespecified VR as non-inferior to Kalinox® with a margin of 3 points. Self-reported pain and anxiety were also analysed using numeric rate scale (NRS).
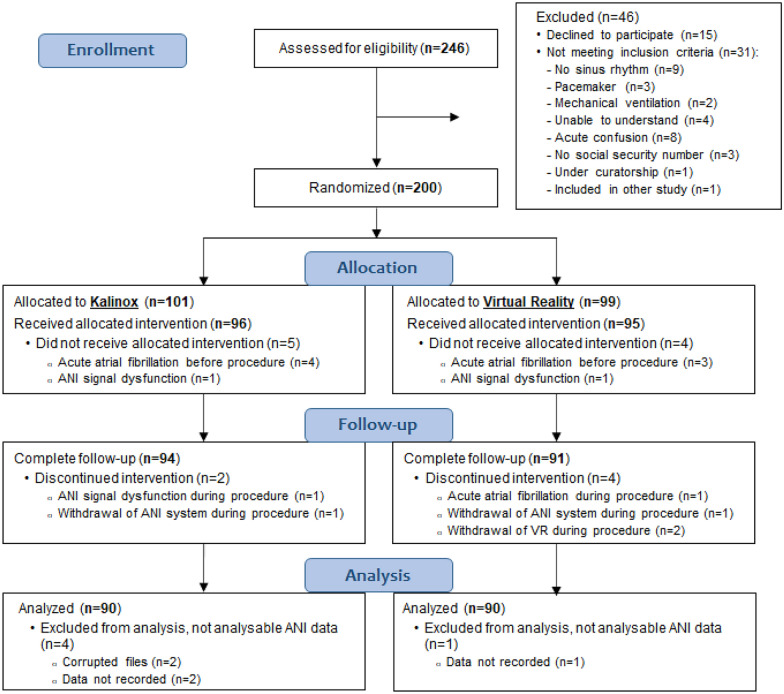
200 patients were included, 99 in the VR group and 101 in the Kalinox® group; 90 patients were analysed in both groups in per-protocol analysis. The median age was 68.0 years [60.0-74.8]. The ΔANI was - 15.1 ± 12.9 in the Kalinox® group and - 15.7 ± 11.6 in the VR group (NS). The mean difference was, therefore, - 0.6 [- 3.6 to 2.4], including the non-inferiority margin of 3. Patients in the VR group had a significantly higher pain NRS scale immediately after the drain removal, 5.0 [3.0-7.0] vs. 3.0 [2.0-6.0], p = 0.009, but no difference 10 min after. NRS of anxiety did not differ between the two groups.
Based on the ANI, the current study showed that VR did not reach the statistical requirements for a proven non-inferiority vs. Kalinox® in managing pain and anxiety during chest drain removal. Moreover, VR was less effective based on NRS. More studies are needed to determine if VR might have a place in the overall approach to pain and anxiety in intensive care units. Trial registration NCT, NCT03956264. Registered 20 May 2019, https://clinicaltrials.gov/ct2/show/NCT03956264.
疼痛和焦虑的管理在重症监护病房仍然是一项挑战。通过分散患者注意力,虚拟现实(VR)可能在疼痛性操作中发挥作用。我们比较了VR与吸入等摩尔比的一氧化氮和氧气混合物(Kalinox®)在心脏手术后拔除胸管期间对疼痛和焦虑的管理效果。
前瞻性、非劣效性、开放标签研究。患者在拔除胸管时被随机分配接受Kalinox®或VR治疗。在操作过程中监测镇痛/伤害感受指数(ANI)以客观评估疼痛和焦虑。主要终点是基于ANIm(4分钟平均值)的操作过程中的ΔANI(ANI - ANI)。我们预先设定VR不劣于Kalinox®,差值为3分。还使用数字评分量表(NRS)分析了自我报告的疼痛和焦虑情况。
纳入200例患者,VR组99例,Kalinox®组101例;在符合方案分析中,两组各有90例患者进行了分析。中位年龄为68.0岁[60.0 - 74.8]。Kalinox®组的ΔANI为 - 15.1±12.9,VR组为 - 15.7±11.6(无统计学差异)。因此,平均差值为 - 0.6[-3.6至2.4],包括3分的非劣效性差值。VR组患者在拔除胸管后立即的疼痛NRS评分显著更高,为5.0[3.0 - 7.0],而Kalinox®组为3.0[2.0 - 6.0],p = 0.009,但10分钟后无差异。两组焦虑的NRS评分无差异。
基于ANI,当前研究表明VR在心脏手术后拔除胸管期间管理疼痛和焦虑方面未达到与Kalinox®相比经证实的非劣效性的统计要求。此外,基于NRS,VR效果较差。需要更多研究来确定VR在重症监护病房疼痛和焦虑的整体管理方法中是否有一席之地。试验注册号NCT,NCT03956264。于2019年5月20日注册,https://clinicaltrials.gov/ct2/show/NCT03956264 。