Department of Cardiology, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200, Aarhus N, Denmark.
Department of Cardiology, Odense University Hospital, Odense, Denmark.
Crit Care. 2021 May 22;25(1):174. doi: 10.1186/s13054-021-03606-5.
Mechanical circulatory support (MCS) with either extracorporeal membrane oxygenation or Impella has shown potential as a salvage therapy for patients with refractory out-of-hospital cardiac arrest (OHCA). The objective of this study was to describe the gradual implementation, survival and adherence to the national consensus with respect to use of MCS for OHCA in Denmark, and to identify factors associated with outcome.
This retrospective, observational cohort study included patients receiving MCS for OHCA at all tertiary cardiac arrest centers (n = 4) in Denmark between July 2011 and December 2020. Logistic regression and Kaplan-Meier survival analysis were used to determine association with outcome. Outcome was presented as survival to hospital discharge with good neurological outcome, 30-day survival and predictors of 30-day mortality.
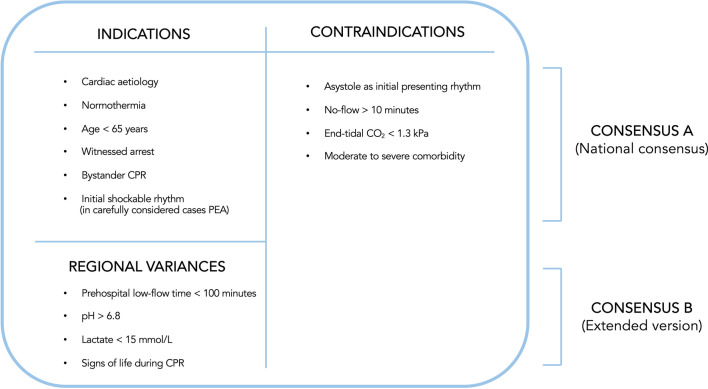
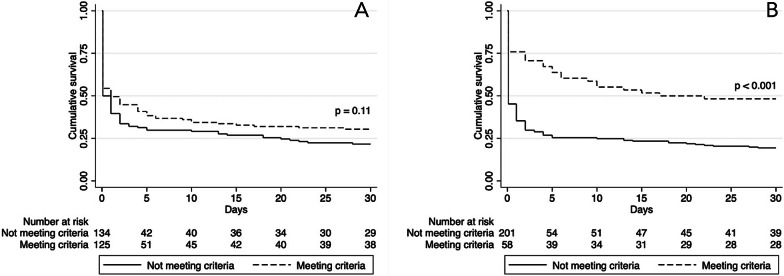
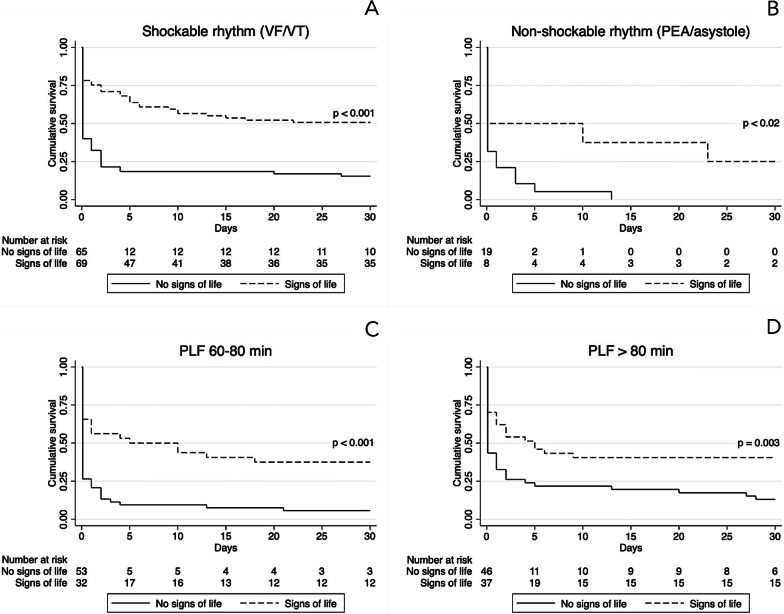
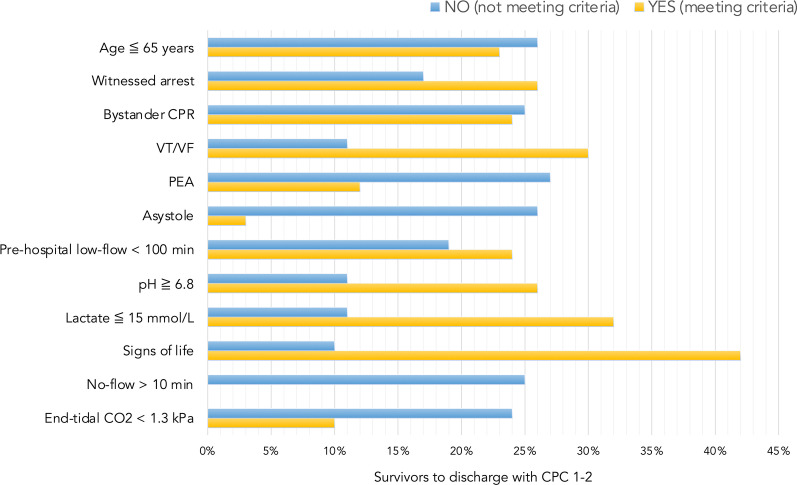
A total of 259 patients were included in the study. Thirty-day survival was 26%. Sixty-five (25%) survived to hospital discharge and a good neurological outcome (Glasgow-Pittsburgh Cerebral Performance Categories 1-2) was observed in 94% of these patients. Strict adherence to the national consensus showed a 30-day survival rate of 30% compared with 22% in patients violating one or more criteria. Adding criteria to the national consensus such as signs of life during cardiopulmonary resuscitation (CPR), pre-hospital low-flow < 100 min, pH > 6.8 and lactate < 15 mmol/L increased the survival rate to 48%, but would exclude 58% of the survivors from the current cohort. Logistic regression identified asystole (RR 1.36, 95% CI 1.18-1.57), pulseless electrical activity (RR 1.20, 95% CI 1.03-1.41), initial pH < 6.8 (RR 1.28, 95% CI 1.12-1.46) and lactate levels > 15 mmol/L (RR 1.16, 95% CI 1.16-1.53) as factors associated with increased risk of 30-day mortality. Patients presenting signs of life during CPR had reduced risk of 30-day mortality (RR 0.63, 95% CI 0.52-0.76).
A high survival rate with a good neurological outcome was observed in this Danish population of patients treated with MCS for OHCA. Stringent patient selection for MCS may produce higher survival rates but potentially withholds life-saving treatment in a significant proportion of survivors.
体外膜肺氧合或 Impella 等机械循环支持已显示出作为难治性院外心脏骤停(OHCA)患者抢救治疗的潜力。本研究的目的是描述丹麦使用机械循环支持治疗 OHCA 的国家共识的逐步实施、生存情况和遵守情况,并确定与结果相关的因素。
这是一项回顾性、观察性队列研究,纳入了 2011 年 7 月至 2020 年 12 月期间丹麦所有三级心脏骤停中心(n=4)接受 OHCA 机械循环支持治疗的患者。使用逻辑回归和 Kaplan-Meier 生存分析来确定与结果的关联。结果以出院时生存且神经功能良好、30 天生存和 30 天死亡率预测因素的比例表示。
本研究共纳入 259 例患者。30 天生存率为 26%。65 例(25%)存活至出院,其中 94%的患者神经功能良好(格拉斯哥-匹兹堡脑功能表现分类 1-2 级)。严格遵守国家共识的患者 30 天生存率为 30%,而违反一条或多条标准的患者为 22%。将生命迹象、心肺复苏前低灌注<100min、pH>6.8 和乳酸<15mmol/L 等标准添加到国家共识中,可将生存率提高至 48%,但会将当前队列中的 58%的幸存者排除在外。逻辑回归确定停搏(RR 1.36,95%CI 1.18-1.57)、无脉性电活动(RR 1.20,95%CI 1.03-1.41)、初始 pH<6.8(RR 1.28,95%CI 1.12-1.46)和乳酸水平>15mmol/L(RR 1.16,95%CI 1.16-1.53)是与 30 天死亡率增加相关的因素。在 CPR 期间出现生命迹象的患者 30 天死亡率降低(RR 0.63,95%CI 0.52-0.76)。
本丹麦 OHCA 患者机械循环支持治疗的生存结果良好,具有较高的生存率。对 MCS 进行严格的患者选择可能会提高生存率,但可能会使相当一部分幸存者失去救命治疗。