Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, Liverpool, United Kingdom.
Anthem Inc., Indianapolis, IN, USA.
Eur J Intern Med. 2021 Sep;91:53-58. doi: 10.1016/j.ejim.2021.04.023. Epub 2021 May 14.
The elderly multi-morbid patient is at high risk of adverse outcomes with COVID-19 complications, and in the general population, the development of incident AF is associated with worse outcomes in such patients. There is therefore the need to identify those patients with COVID-19 who are at highest risk of developing incident AF. We therefore investigated incident AF risks in a large prospective population of elderly patients with/without incident COVID-19 cases and baseline cardiovascular/non-cardiovascular multi-morbidities. We used two approaches: main effect modeling and secondly, a machine-learning (ML) approach, accounting for the complex dynamic relationships among comorbidity variables.
We studied a prospective elderly US cohort of 280,592 patients from medical databases in an 8-month investigation of with/without newly incident COVID19 cases. Incident AF outcomes were examined in relationship to diverse multi-morbid conditions, COVID-19 status and demographic variables, with ML accounting for the dynamic nature of changing multimorbidity risk factors.
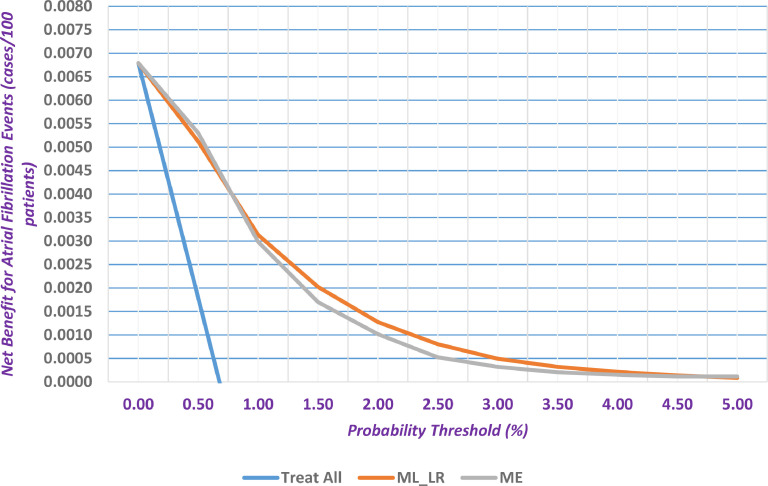
Multi-morbidity contributed to the onset of confirmed COVID-19 cases with cognitive impairment (OR 1.69; 95%CI 1.52-1.88), anemia (OR 1.41; 95%CI 1.32-1.50), diabetes mellitus (OR 1.35; 95%CI 1.27-1.44) and vascular disease (OR 1.30; 95%CI 1.21-1.39) having the highest associations. A main effect model (C-index value 0.718) showed that COVID-19 had the highest association with incident AF cases (OR 3.12; 95%CI 2.61-3.710, followed by congestive heart failure (1.72; 95%CI 1.50-1.96), then coronary artery disease (OR 1.43; 95%CI 1.27-1.60) and valvular disease (1.42; 95%CI 1.26-1.60). The ML algorithm demonstrated improved discriminatory validity incrementally over the statistical main effect model (training: C-index 0.729, 95%CI 0.718-0.740; validation: C-index 0.704, 95%CI 0.687-0.72). Calibration of the ML based formulation was satisfactory and better than the main-effect model. Decision curve analysis demonstrated that the clinical utility for the ML based formulation was better than the 'treat all' strategy and the main effect model.
COVID-19 status has major implications for incident AF in a cohort with diverse cardiovascular/non-cardiovascular multi-morbidities. Our ML approach accounting for dynamic multimorbidity changes had good prediction for new onset AF amongst incident COVID19 cases.
患有多种合并症的老年患者感染 COVID-19 后发生不良后果的风险较高,而在一般人群中,新发房颤的发生与此类患者的预后较差相关。因此,需要识别出感染 COVID-19 的患者中发生新发房颤风险最高的患者。因此,我们在一个包含患有/不患有 COVID-19 的新发病例的、有大量老年患者的前瞻性队列中,研究了新发房颤的风险,并对基线心血管/非心血管合并症进行了研究。我们使用了两种方法:主要效应模型和其次,机器学习 (ML) 方法,同时考虑了合并症变量之间的复杂动态关系。
我们研究了来自医疗数据库的 280592 名美国老年患者的前瞻性队列,对 8 个月内有无新发 COVID19 病例进行了研究。分析了新发房颤结局与多种合并症、COVID-19 状况和人口统计学变量之间的关系,机器学习方法同时考虑了合并症危险因素的动态变化。
合并症导致确诊 COVID-19 病例的发生,其中认知障碍(OR 1.69;95%CI 1.52-1.88)、贫血(OR 1.41;95%CI 1.32-1.50)、糖尿病(OR 1.35;95%CI 1.27-1.44)和血管疾病(OR 1.30;95%CI 1.21-1.39)的相关性最高。主要效应模型(C 指数值 0.718)显示,COVID-19 与新发房颤病例的相关性最高(OR 3.12;95%CI 2.61-3.710),其次是充血性心力衰竭(1.72;95%CI 1.50-1.96),其次是冠心病(OR 1.43;95%CI 1.27-1.60)和瓣膜疾病(OR 1.42;95%CI 1.26-1.60)。ML 算法显示出优于统计主要效应模型的增量判别有效性(训练:C 指数 0.729,95%CI 0.718-0.740;验证:C 指数 0.704,95%CI 0.687-0.72)。基于 ML 的公式的校准是令人满意的,并且优于主要效应模型。决策曲线分析表明,基于 ML 的公式的临床实用性优于“治疗所有”策略和主要效应模型。
COVID-19 状态对伴有多种心血管/非心血管合并症的患者新发房颤有重要影响。我们的 ML 方法同时考虑了合并症的动态变化,对新发 COVID19 病例中新发房颤的发生有较好的预测作用。