Clinical Psychology in Healthcare, Department of Women's and Children's Health, Uppsala University, Uppsala, Sweden.
Centre for Psychiatry Research, Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden.
J Med Internet Res. 2021 May 24;23(5):e25465. doi: 10.2196/25465.
The U-CARE Heart trial was one of the first randomized controlled trials to evaluate the effect of internet-based cognitive behavioral therapy on self-reported symptoms of anxiety or depression for patients with a recent myocardial infarction. While the effects of internet-based cognitive behavioral therapy on Hospital Anxiety and Depression Scale (HADS) scores at 14 weeks postbaseline were not significant, in this study, we investigated possible long-term effects of treatment.
The aim of this study was to evaluate the long-term effectiveness of internet-based cognitive behavioral therapy on self-reported symptoms of anxiety and depression in patients 12 months after a myocardial infarction and to explore subsequent occurrences of cardiovascular disease events.
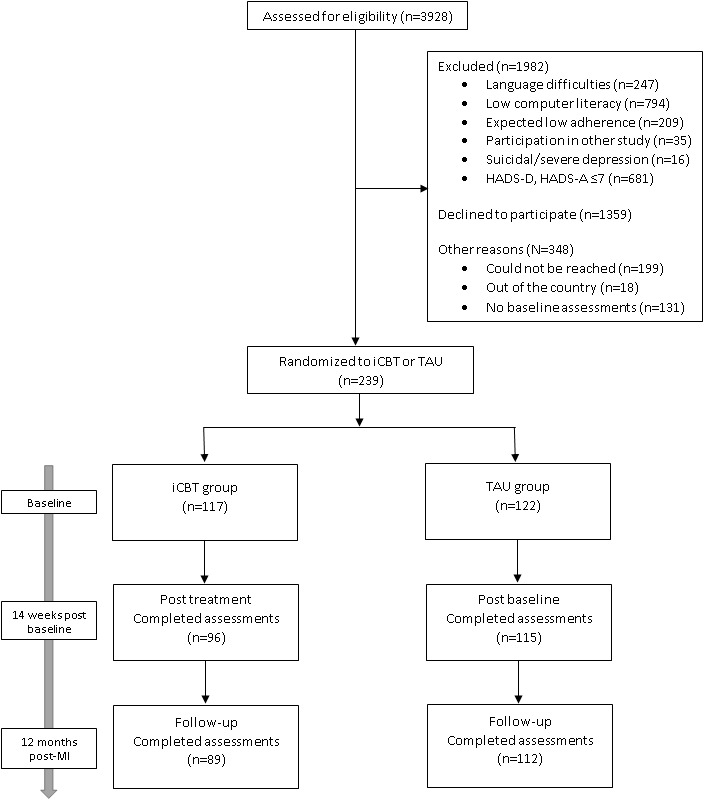
Shortly after acute myocardial infarction, 239 patients (33% female, mean age 59.6 years) reporting mild-to-moderate symptoms of anxiety or depression were randomized to 14 weeks of therapist-guided internet-based cognitive behavioral therapy (n=117) or treatment as usual (n=122). Data from national registries were used to explore group differences in clinical outcomes such as cardiovascular disease and cardiovascular-related mortality for a follow-up period of up to 5 years: group differences in HADS total score 1 year post-myocardial infarction, the primary outcome, was analyzed using multiple linear regression. Secondary outcomes, such as HADS anxiety and depression subscales and the Cardiac Anxiety Questionnaire total score (CAQ), which measures heart-focused anxiety, were analyzed in the same way. Multiple imputation was used to account for missing data, and a pooled treatment effect was estimated. Adjusted Cox proportional hazards models were used to estimate hazard ratios (HRs) for data pertaining to registry outcomes.
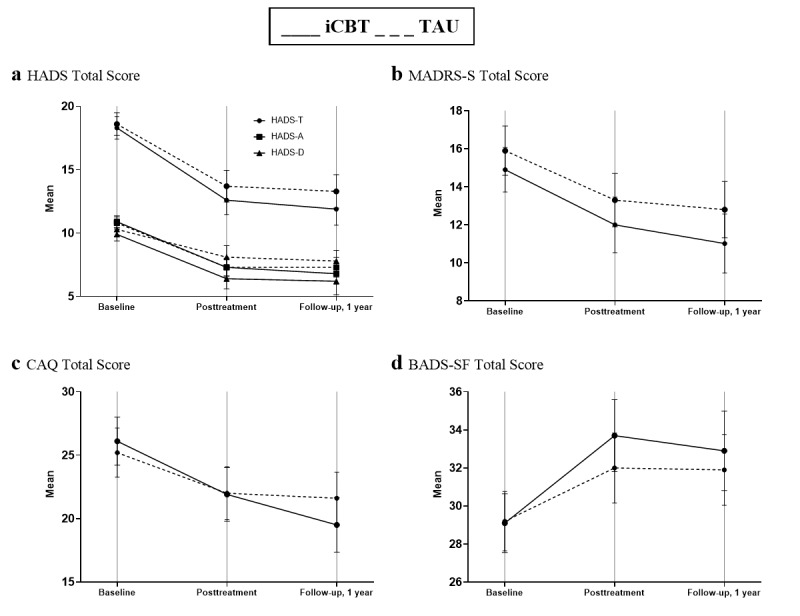
Both groups reported lower HADS total scores 1 year after myocardial infarction than those at baseline. HADS total scores were not significantly different between the treatment and control groups 1 year after myocardial infarction (β=-1.14, 95% CI -2.73 to 0.45, P=.16). CAQ was the only measure improved significantly by internet-based cognitive behavioral therapy when compared with treatment as usual (β=-2.58, 95% CI -4.75 to -0.42, P=.02) before adjusting for multiple comparisons. The composite outcome of nonfatal cardiovascular events and cardiovascular-related mortality did not differ between groups but was numerically higher in the internet-based cognitive behavioral therapy group, who were at slightly greater risk (HR 1.8, 95% CI 0.96 to 3.4, P=.07). Adjusting for previous myocardial infarction and diabetes attenuated this estimate (HR 1.5, 95% CI 0.8 to 2.8, P=.25).
Internet-based cognitive behavioral therapy was not superior in reducing self-reported symptoms of depression or anxiety compared to treatment as usual at the 1-year follow-up after myocardial infarction. A reduction in cardiac-related anxiety was observed but was not significant after adjusting for multiple comparisons. There was no difference in risk of cardiovascular events between the treatment groups. Low treatment adherence, which might have affected treatment engagement and outcomes, should be considered when interpreting these results.
ClinicalTrials.gov NCT01504191; https://clinicaltrials.gov/ct2/show/NCT01504191.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): RR2-10.1186/s13063-015-0689-y.
U-CARE 心脏试验是第一项评估基于互联网的认知行为疗法对近期心肌梗死患者焦虑或抑郁的自我报告症状影响的随机对照试验之一。虽然基于互联网的认知行为疗法对基线后 14 周 HADS 评分的影响没有统计学意义,但在本研究中,我们研究了治疗的可能长期效果。
本研究旨在评估心肌梗死后 12 个月内基于互联网的认知行为疗法对患者焦虑和抑郁的自我报告症状的长期有效性,并探讨随后发生的心血管疾病事件。
急性心肌梗死后不久,239 名(33%为女性,平均年龄 59.6 岁)报告有轻度至中度焦虑或抑郁症状的患者被随机分为 14 周的治疗师指导的基于互联网的认知行为疗法组(n=117)或常规治疗组(n=122)。使用国家登记数据探讨组间差异,如心血管疾病和心血管相关死亡率的临床结局:心肌梗死后 1 年的主要结局 HADS 总分的组间差异使用多元线性回归进行分析。以同样的方式分析 HADS 焦虑和抑郁分量表和测量心脏相关焦虑的心脏焦虑问卷(CAQ)总分等次要结局。使用多重插补来处理缺失数据,并估计了合并治疗效果。调整 Cox 比例风险模型估计与登记结局相关的数据的危险比(HR)。
两组患者在心肌梗死后 1 年时的 HADS 总分均低于基线时。心肌梗死后 1 年时,治疗组和对照组之间的 HADS 总分无显著差异(β=-1.14,95%CI-2.73 至 0.45,P=.16)。在进行多次比较调整之前,CAQ 是唯一一项与常规治疗相比显著改善的测量指标(β=-2.58,95%CI-4.75 至-0.42,P=.02)。非致命性心血管事件和心血管相关死亡率的复合结局在两组之间没有差异,但基于互联网的认知行为疗法组的发生率略高,风险略高(HR 1.8,95%CI 0.96 至 3.4,P=.07)。调整先前的心肌梗死和糖尿病后,该估计值减弱(HR 1.5,95%CI 0.8 至 2.8,P=.25)。
与常规治疗相比,基于互联网的认知行为疗法在心肌梗死后 1 年的随访中并没有降低抑郁或焦虑的自我报告症状。观察到心脏相关焦虑的减少,但在进行多次比较调整后并不显著。两组之间心血管事件的风险没有差异。在解释这些结果时,应考虑到低治疗依从性,这可能影响了治疗的参与和结果。
ClinicalTrials.gov NCT01504191;https://clinicaltrials.gov/ct2/show/NCT01504191.
国际注册报告标识符(IRRID):RR2-10.1186/s13063-015-0689-y。