Department of Health Law, Policy, and Management, Boston University School of Public Health, Boston, MA, USA.
Grayken Center for Addiction, Clinical Addiction Research and Education Unit, Section of General Internal Medicine, Department of Medicine, Boston Medical Center and Boston University School of Medicine, Boston, MA, USA.
Drug Alcohol Depend. 2021 Aug 1;225:108764. doi: 10.1016/j.drugalcdep.2021.108764. Epub 2021 May 21.
While the United States is in the midst of an overdose epidemic, effective treatments are underutilized and commonly discontinued. Innovations in medication delivery, including an extended-release formulations, have the potential to improve treatment access and reduce discontinuation. We sought to assess extended-release buprenorphine discontinuation among individuals with opioid use disorder (OUD) in a real-world, nationally representative cohort.
United States PARTICIPANTS: Commercially insured individuals initiating one of four FDA-approved medications for opioid use disorder (MOUD) in 2018: extended-release buprenorphine, extended-release naltrexone, mucosal buprenorphine (mono- or co-formulated with naloxone), or methadone.
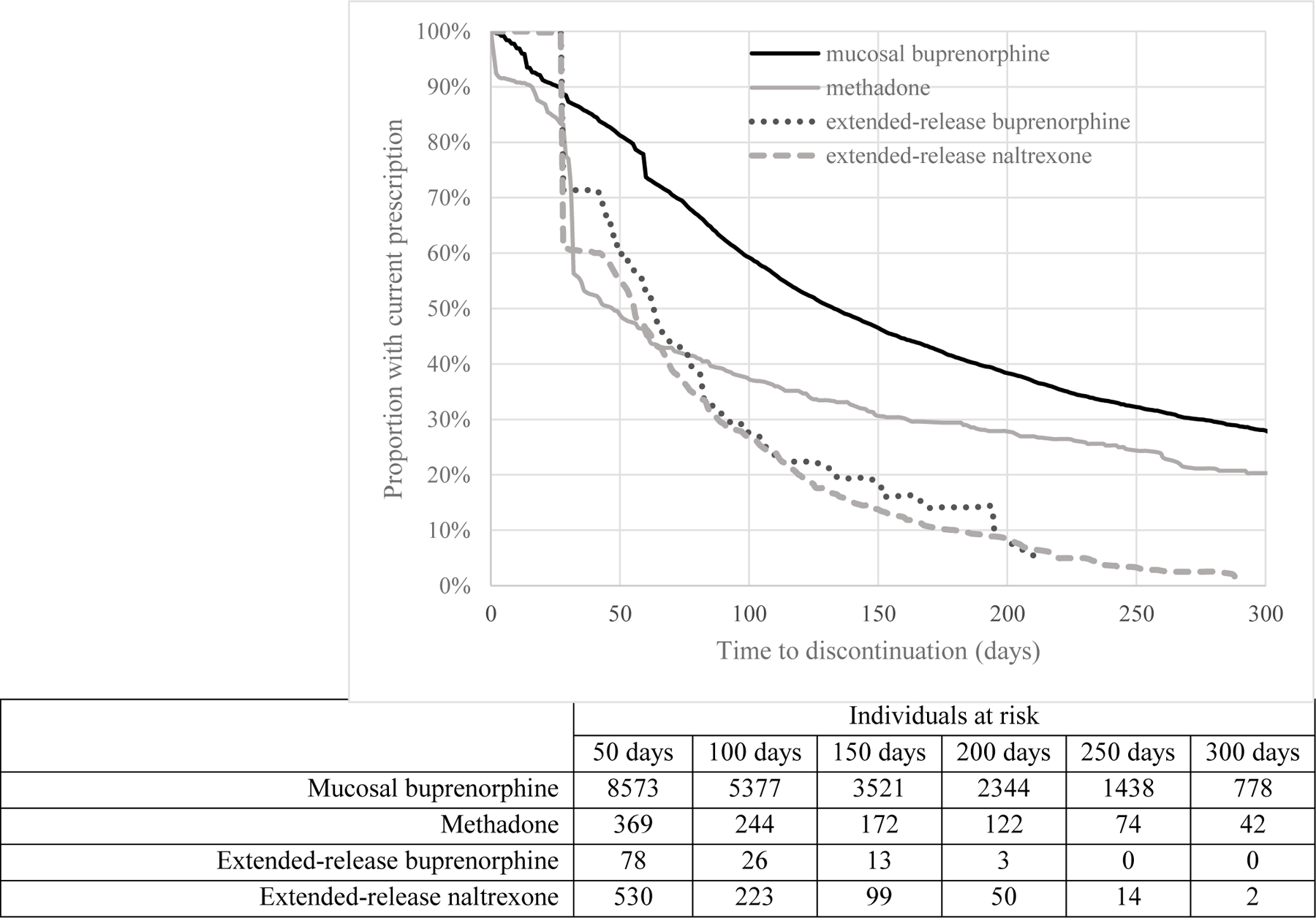
Our primary outcome was medication discontinuation, defined as a gap of more than 14 days between the end of one prescription or administration and the subsequent dose.
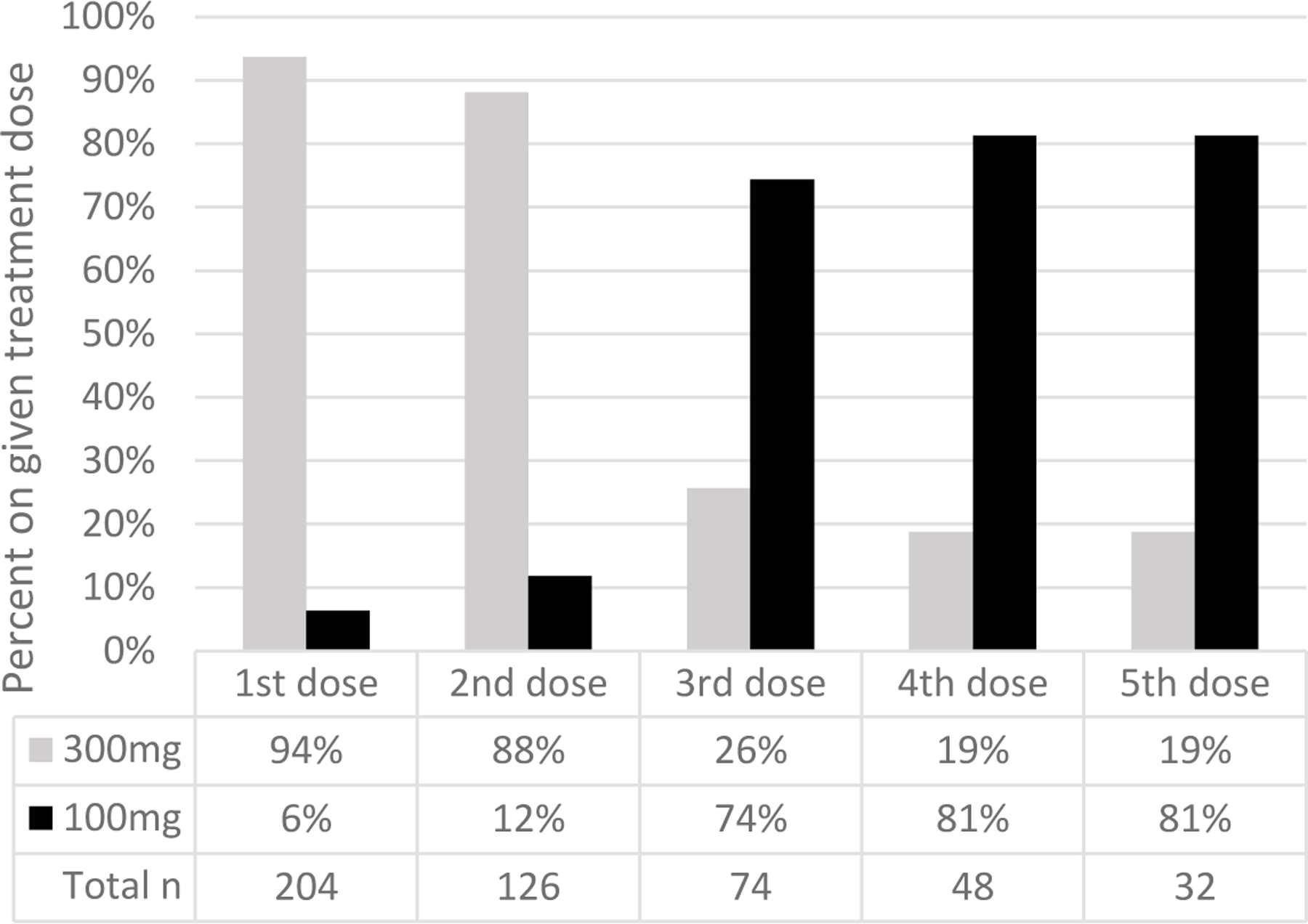
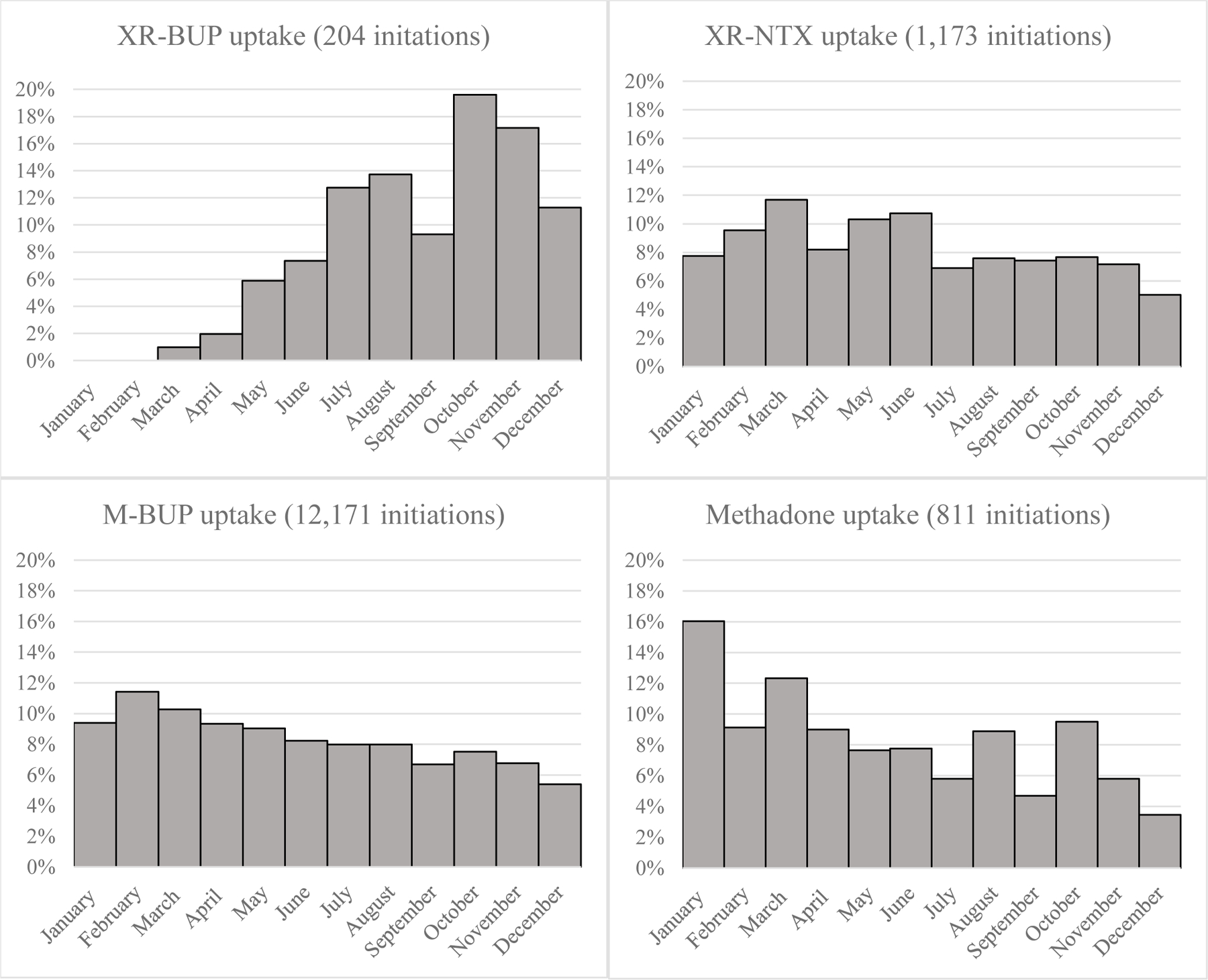
We identified 14,358 individuals initiating MOUD in 2018, including 204 (1%) extended-release buprenorphine, 1,173 (8%) extended-release naltrexone, 12,171 (85%) mucosal buprenorphine, and 810 (6%) methadone initiations. Three months after initiation, 50% (95% confidence interval [CI] 40%-60%) of extended-release buprenorphine, 64% (95% CI 61%-69%) of extended-release naltrexone, 34% (95% CI 33%-35%) of mucosal buprenorphine, and 58% (95% CI 54%-62%) of methadone initiators had discontinued treatment.
Across all treatment groups, medication discontinuation was high, and in this sample of early adopters with limited follow-up time, we found no evidence that extended-release buprenorphine offered a retention advantage compared to other MOUD in real-world settings. Retention continues to represent a major obstacle to treatment effectiveness, and interventions are needed to address this challenge even as new MOUD formulations become available.
在美国正处于阿片类药物过量流行之际,有效的治疗方法未得到充分利用,且通常会被中断。药物输送方面的创新,包括延长释放制剂,有可能改善治疗的可及性并减少中断。我们旨在评估在真实世界中具有代表性的、接受阿片类药物使用障碍(OUD)治疗的个体中,延长释放丁丙诺啡的停药情况。
美国
2018 年接受四种 FDA 批准的阿片类药物使用障碍治疗药物(MOUD)之一的商业保险个体:延长释放丁丙诺啡、延长释放纳曲酮、黏膜丁丙诺啡(与纳洛酮单药或联合配方)或美沙酮。
我们的主要结局是药物停药,定义为一种处方或给药结束后与随后剂量之间超过 14 天的空白期。
我们确定了 2018 年开始 MOUD 的 14358 人,其中包括 204 名(1%)延长释放丁丙诺啡、1173 名(8%)延长释放纳曲酮、12171 名(85%)黏膜丁丙诺啡和 810 名(6%)美沙酮。在开始治疗后 3 个月,50%(95%置信区间 [CI] 40%-60%)的延长释放丁丙诺啡、64%(95% CI 61%-69%)的延长释放纳曲酮、34%(95% CI 33%-35%)的黏膜丁丙诺啡和 58%(95% CI 54%-62%)的美沙酮开始者停止了治疗。
在所有治疗组中,药物停药率都很高,在这个接受治疗时间有限的早期采用者样本中,我们没有发现证据表明,与其他 MOUD 相比,延长释放丁丙诺啡在真实环境中具有保留优势。保留仍然是治疗效果的主要障碍,即使新的 MOUD 制剂可用,也需要采取干预措施来应对这一挑战。