Department of General Surgery, Guthrie Robert Packer Hospital, 1 Guthrie Square, Sayre, PA, 18840, USA.
, Seattle, WA, USA.
Sci Rep. 2021 Jun 4;11(1):11832. doi: 10.1038/s41598-021-90100-1.
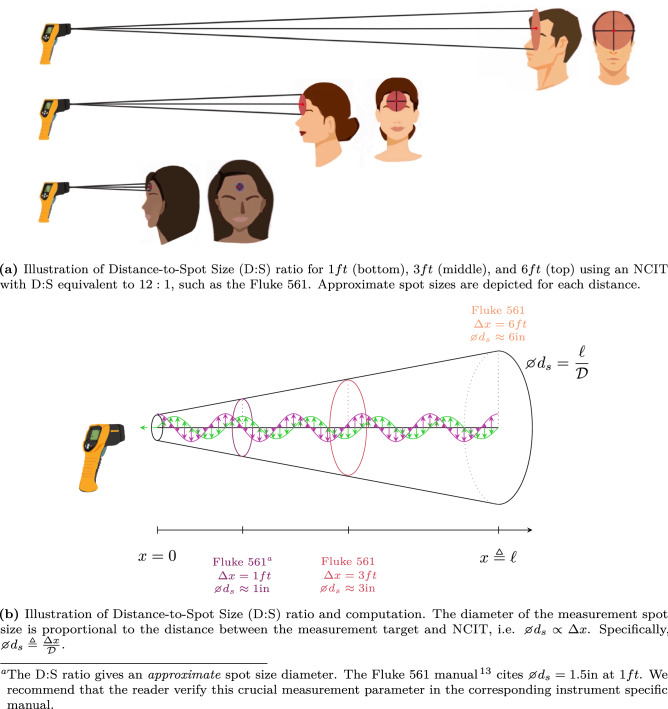
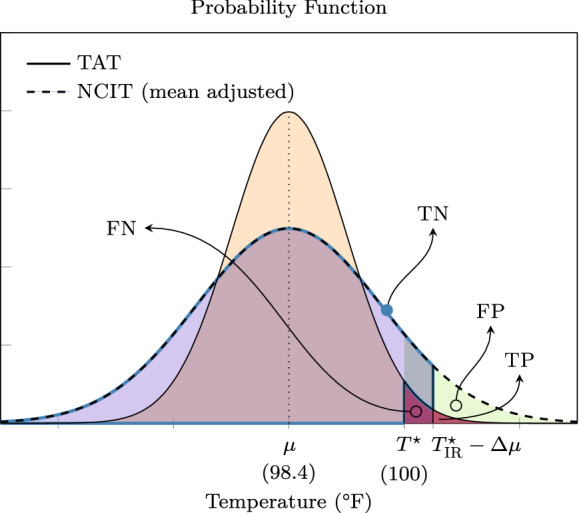
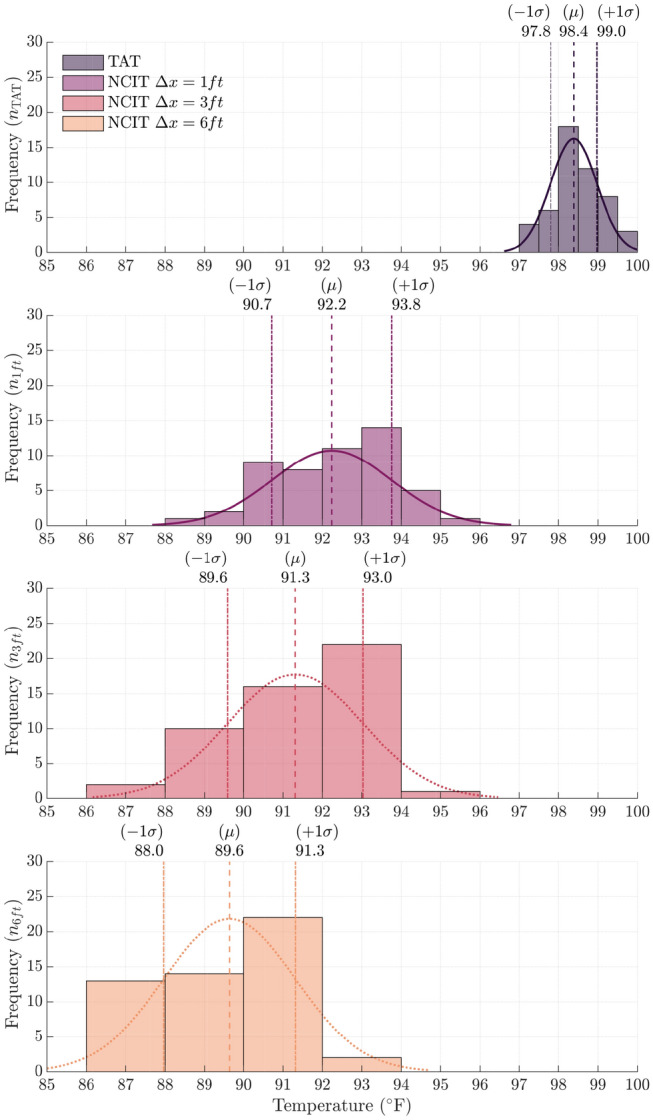
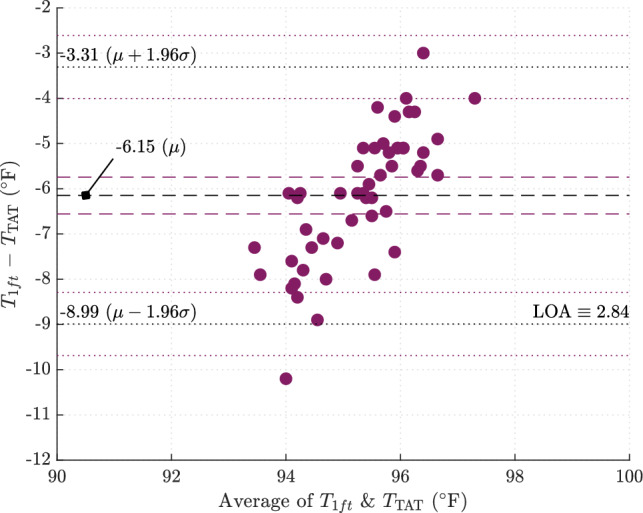
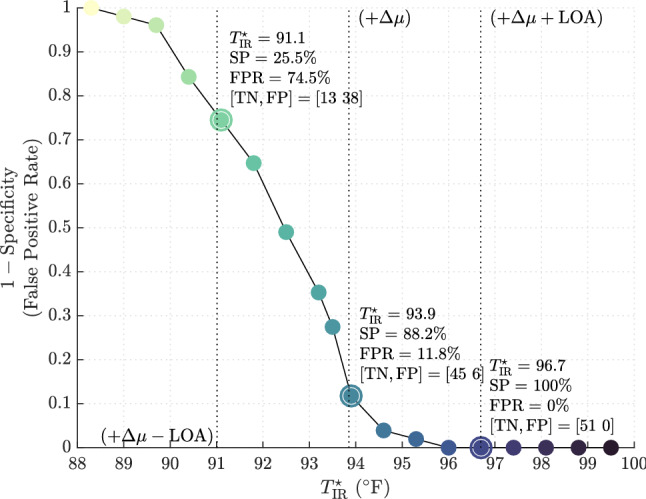
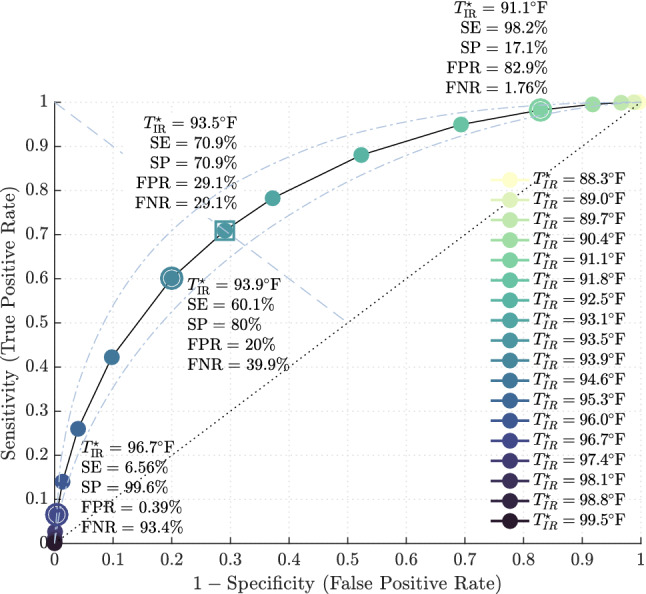
Among the myriad of challenges healthcare institutions face in dealing with coronavirus disease 2019 (COVID-19), screening for the detection of febrile persons entering facilities remains problematic, particularly when paired with CDC and WHO spatial distancing guidance. Aggressive source control measures during the outbreak of COVID-19 has led to re-purposed use of noncontact infrared thermometry (NCIT) for temperature screening. This study was commissioned to establish the efficacy of this technology for temperature screening by healthcare facilities. We conducted a prospective, observational, single-center study in a level II trauma center at the onset of the COVID-19 outbreak to assess (i) method agreement between NCIT and temporal artery reference temperature, (ii) diagnostic accuracy of NCIT in detecting referent temperature [Formula: see text] and ensuing test sensitivity and specificity and (iii) technical limitations of this technology. Of 51 healthy, non-febrile, healthcare workers surveyed, the mean temporal artery temperature was [Formula: see text] ([Formula: see text] confidence interval (CI) = [Formula: see text]). Mean NCIT temperatures measured from [Formula: see text], [Formula: see text], and [Formula: see text] distances were [Formula: see text] [Formula: see text], [Formula: see text] [Formula: see text], and [Formula: see text] [Formula: see text], respectively. From statistical analysis, the only method in sufficient agreement with the reference standard was NCIT at [Formula: see text]. This demonstrated that the device offset (mean temperature difference) between these methods was [Formula: see text] ([Formula: see text]) with 95% of measurement differences within [Formula: see text] ([Formula: see text]) and [Formula: see text] ([Formula: see text]). By setting the NCIT screening threshold to [Formula: see text] at [Formula: see text], we achieve diagnostic accuracy with [Formula: see text] test sensitivity and specificity for temperature detection [Formula: see text] by reference standard. In comparison, reducing this screening criterion to the lower limit of the device-specific offset, such as [Formula: see text], produces a highly sensitive screening test at [Formula: see text], which may be favorable in high-risk pandemic disease. For future consideration, an infrared device with a higher distance-to-spot size ratio approaching 50:1 would theoretically produce similar results at [Formula: see text], in accordance with CDC and WHO spatial distancing guidelines.
在医疗机构应对 2019 年冠状病毒病(COVID-19)的诸多挑战中,对进入设施的发热人员进行筛查仍然存在问题,尤其是与疾病预防控制中心(CDC)和世界卫生组织(WHO)的空间距离指导相结合时。在 COVID-19 爆发期间采取了积极的源控制措施,导致重新使用非接触式红外测温仪(NCIT)进行体温筛查。这项研究是为了确定医疗机构使用这项技术进行体温筛查的效果。我们在 COVID-19 爆发开始时在二级创伤中心进行了一项前瞻性、观察性、单中心研究,以评估(i)NCIT 与颞动脉参考温度之间的方法一致性,(ii)NCIT 在检测参考温度 [Formula: see text]时的诊断准确性以及随后的测试灵敏度和特异性,以及(iii)该技术的技术限制。在 51 名健康、无发热的医护人员中进行了调查,颞动脉的平均温度为 [Formula: see text]([Formula: see text]置信区间[CI] = [Formula: see text])。从 [Formula: see text]、[Formula: see text] 和 [Formula: see text] 距离测量的平均 NCIT 温度分别为 [Formula: see text]、[Formula: see text] 和 [Formula: see text]。从统计学分析来看,与参考标准足够一致的唯一方法是 NCIT 在 [Formula: see text]。这表明,这些方法之间的设备偏移量(平均温差)为 [Formula: see text]([Formula: see text]),95%的测量差值在 [Formula: see text]([Formula: see text])和 [Formula: see text]([Formula: see text])范围内。将 NCIT 筛查阈值设置为 [Formula: see text] 在 [Formula: see text],我们可以达到 [Formula: see text]的诊断准确性,测试灵敏度和特异性为 [Formula: see text]由参考标准检测。相比之下,将此筛查标准降低到设备特定偏移量的下限,例如 [Formula: see text],则在 [Formula: see text] 时产生高度敏感的筛查测试,这在高风险大流行疾病中可能是有利的。未来需要考虑的是,具有更接近 50:1 的距离-光斑尺寸比的红外设备在 [Formula: see text] 时理论上会产生类似的结果,这符合疾病预防控制中心(CDC)和世界卫生组织(WHO)的空间距离指南。