Ferreira Juliana C, Ho Yeh-Li, Besen Bruno Adler Maccagnan Pinheiro, Malbouisson Luiz Marcelo Sa, Taniguchi Leandro Utino, Mendes Pedro Vitale, Costa Eduardo Leite Vieira, Park Marcelo, Daltro-Oliveira Renato, Roepke Roberta M L, Silva-Jr Joao M, Carmona Maria Jose Carvalho, Carvalho Carlos R R
Divisao de Pneumologia, Instituto Do Coracao, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, São Paulo, Brazil.
Intensive Care Unit, AC Camargo Cancer Center, São Paulo, Brazil.
Ann Intensive Care. 2021 Jun 7;11(1):92. doi: 10.1186/s13613-021-00882-w.
Approximately 5% of COVID-19 patients develop respiratory failure and need ventilatory support, yet little is known about the impact of mechanical ventilation strategy in COVID-19. Our objective was to describe baseline characteristics, ventilatory parameters, and outcomes of critically ill patients in the largest referral center for COVID-19 in Sao Paulo, Brazil, during the first surge of the pandemic.
This cohort included COVID-19 patients admitted to the intensive care units (ICUs) of an academic hospital with 94 ICU beds, a number expanded to 300 during the pandemic as part of a state preparedness plan. Data included demographics, advanced life support therapies, and ventilator parameters. The main outcome was 28-day survival. We used a multivariate Cox model to test the association between protective ventilation and survival, adjusting for PF ratio, pH, compliance, and PEEP.
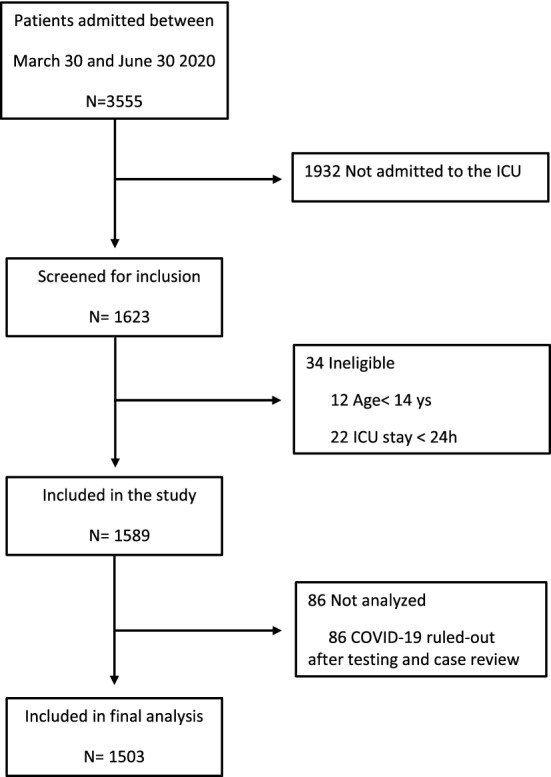
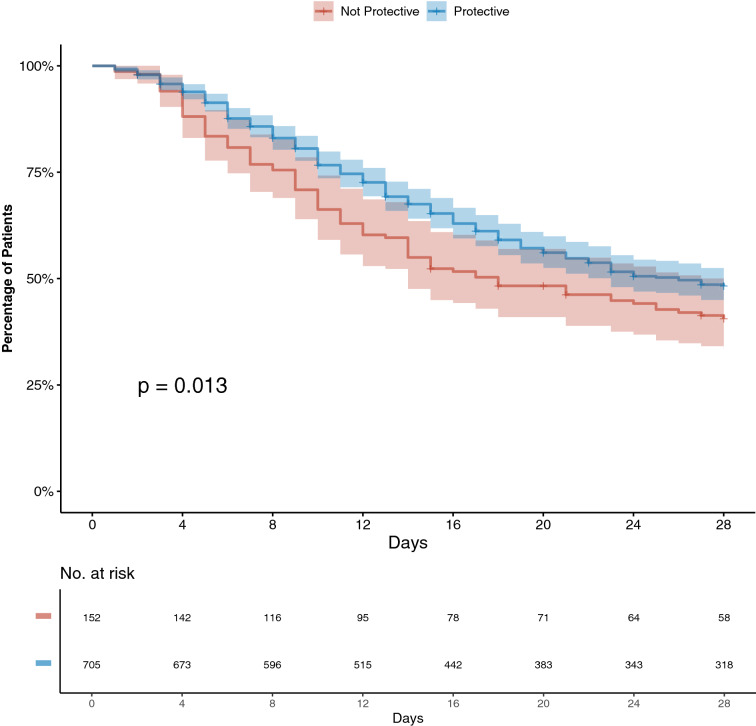
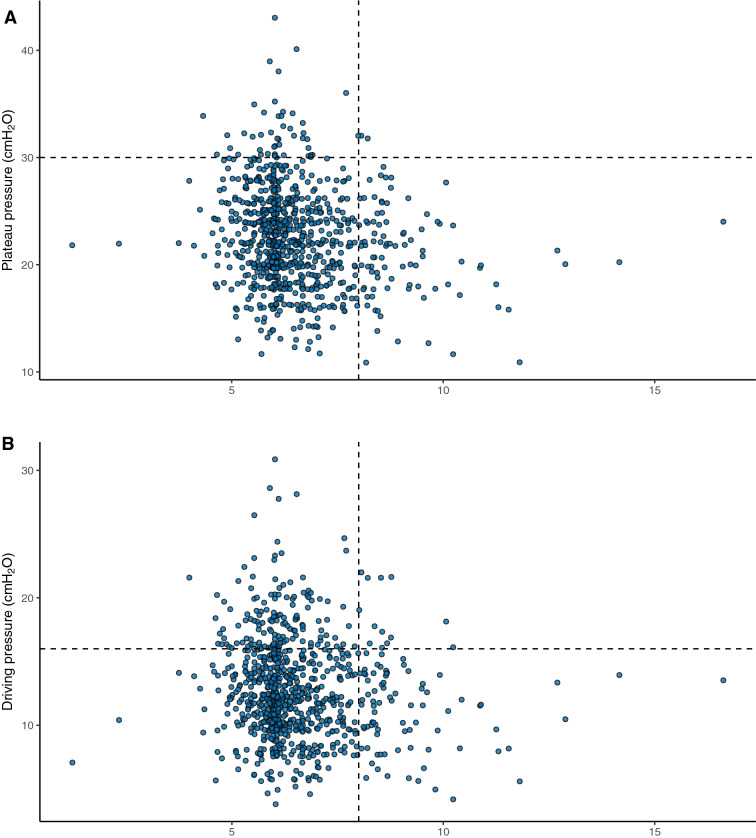
We included 1503 patients from March 30 to June 30, 2020. The mean age was 60 ± 15 years, and 59% were male. During 28-day follow-up, 1180 (79%) patients needed invasive ventilation and 666 (44%) died. For the 984 patients who were receiving mechanical ventilation in the first 24 h of ICU stay, mean tidal volume was 6.5 ± 1.3 mL/kg of ideal body weight, plateau pressure was 24 ± 5 cmHO, respiratory system compliance was 31.9 (24.4-40.9) mL/cmHO, and 82% of patients were ventilated with protective ventilation. Noninvasive ventilation was used in 21% of patients, and prone, in 36%. Compliance was associated with survival and did not show a bimodal pattern that would support the presence of two phenotypes. In the multivariable model, protective ventilation (aHR 0.73 [95%CI 0.57-0.94]), adjusted for PF ratio, compliance, PEEP, and arterial pH, was independently associated with survival.
During the peak of the epidemic in Sao Paulo, critically ill patients with COVID-19 often required mechanical ventilation and mortality was high. Our findings revealed an association between mechanical ventilation strategy and mortality, highlighting the importance of protective ventilation for patients with COVID-19.
约5%的新冠病毒疾病(COVID-19)患者会发展为呼吸衰竭并需要通气支持,但对于机械通气策略在COVID-19中的影响知之甚少。我们的目标是描述巴西圣保罗最大的COVID-19转诊中心在疫情首次激增期间重症患者的基线特征、通气参数和结局。
该队列包括入住一家拥有94张重症监护病房(ICU)床位的学术医院ICU的COVID-19患者,作为州应急计划的一部分,在疫情期间该数字扩大到300张。数据包括人口统计学、高级生命支持治疗和呼吸机参数。主要结局是28天生存率。我们使用多变量Cox模型来检验保护性通气与生存之间的关联,并对氧合指数(PF)、pH值、肺顺应性和呼气末正压(PEEP)进行校正。
我们纳入了2020年3月30日至6月30日期间的1503例患者。平均年龄为60±15岁,59%为男性。在28天的随访期间,1180例(79%)患者需要有创通气,666例(44%)死亡。对于在入住ICU的前24小时内接受机械通气的984例患者,平均潮气量为6.5±1.3ml/理想体重千克,平台压为24±5cmH₂O,呼吸系统顺应性为31.9(24.4 - 40.9)ml/cmH₂O,82%的患者采用保护性通气。21%的患者使用无创通气,36%的患者采用俯卧位通气。肺顺应性与生存相关,且未显示出支持两种表型存在的双峰模式。在多变量模型中,校正PF比值、肺顺应性、PEEP和动脉pH值后,保护性通气(校正风险比[aHR]0.73[95%置信区间(CI)0.57 - 0.94])与生存独立相关。
在圣保罗疫情高峰期,重症COVID-19患者常需要机械通气且死亡率很高。我们的研究结果揭示了机械通气策略与死亡率之间的关联,凸显了保护性通气对COVID-19患者的重要性。