Division of Internal Medicine, Hepatobiliary and Immunoallergic Diseases, IRCCS Azienda Ospedaliero-Universitaria di Bologna, University of Bologna, Bologna 40138, Italy.
Division of Internal Medicine and Immunorheumatology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Center for the Study and Treatment of Autoimmune Diseases of the Liver and Biliary System, University of Bologna, Bologna 40138, Italy.
World J Gastroenterol. 2021 Jun 14;27(22):2994-3009. doi: 10.3748/wjg.v27.i22.2994.
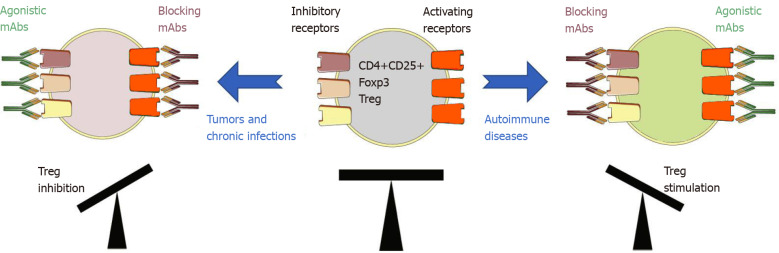
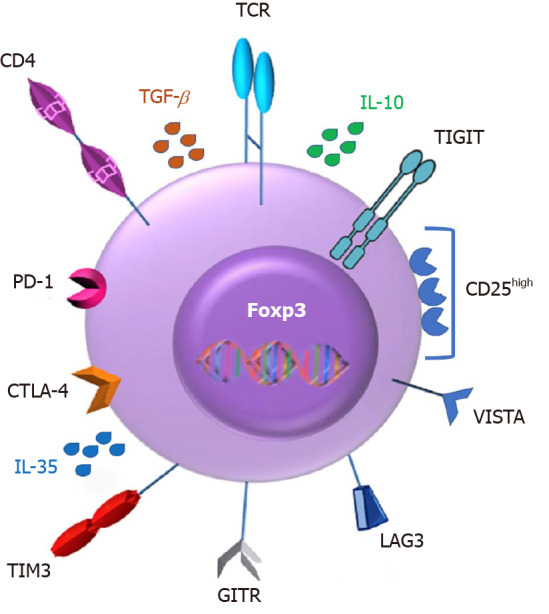
More than 90% of cases of hepatocellular carcinoma (HCC) occurs in patients with cirrhosis, of which hepatitis B virus and hepatitis C virus are the leading causes, while the tumor less frequently arises in autoimmune liver diseases. Advances in understanding tumor immunity have led to a major shift in the treatment of HCC, with the emergence of immunotherapy where therapeutic agents are used to target immune cells rather than cancer cells. Regulatory T cells (Tregs) are the most abundant suppressive cells in the tumor microenvironment and their presence has been correlated with tumor progression, invasiveness, as well as metastasis. Tregs are characterized by the expression of the transcription factor Foxp3 and various mechanisms ranging from cell-to-cell contact to secretion of inhibitory molecules have been implicated in their function. Notably, Tregs amply express checkpoint molecules such as cytotoxic T lymphocyte-associated antigen 4 and programmed cell-death 1 receptor and therefore represent a direct target of immune checkpoint inhibitor (ICI) immunotherapy. Taking into consideration the critical role of Tregs in maintenance of immune homeostasis as well as avoidance of autoimmunity, it is plausible that targeting of Tregs by ICI immunotherapy results in the development of immune-related adverse events (irAEs). Since the use of ICI becomes common in oncology, with an increasing number of new ICI currently under clinical trials for cancer treatment, the occurrence of irAEs is expected to dramatically rise. Herein, we review the current literature focusing on the role of Tregs in HCC evolution taking into account their opposite etiological function in viral and autoimmune chronic liver disease, and we discuss their involvement in irAEs due to the new immunotherapies.
超过 90%的肝细胞癌 (HCC) 发生在肝硬化患者中,其中乙型肝炎病毒和丙型肝炎病毒是主要病因,而自身免疫性肝病中肿瘤较少发生。对肿瘤免疫的深入了解导致 HCC 的治疗发生了重大转变,出现了免疫疗法,即使用治疗药物靶向免疫细胞而不是癌细胞。调节性 T 细胞 (Treg) 是肿瘤微环境中最丰富的抑制性细胞,其存在与肿瘤进展、侵袭性和转移有关。Treg 的特征是转录因子 Foxp3 的表达,并且已经涉及到从细胞间接触到抑制性分子分泌的各种机制在其功能中。值得注意的是,Treg 大量表达检查点分子,如细胞毒性 T 淋巴细胞相关抗原 4 和程序性细胞死亡 1 受体,因此是免疫检查点抑制剂 (ICI) 免疫疗法的直接靶点。考虑到 Treg 在维持免疫稳态和避免自身免疫中的关键作用,ICI 免疫疗法靶向 Treg 可能导致免疫相关不良事件 (irAEs) 的发生。由于 ICI 在肿瘤学中的应用越来越普遍,目前有越来越多的新 ICI 正在临床试验中用于癌症治疗,预计 irAEs 的发生率将大幅上升。在此,我们综述了目前的文献,重点关注 Treg 在 HCC 演变中的作用,同时考虑到它们在病毒性和自身免疫性慢性肝病中的相反病因作用,并讨论了它们在新免疫疗法中因 irAEs 而产生的作用。