Kacew Alec J, Strohbehn Garth W, Saulsberry Loren, Laiteerapong Neda, Cipriani Nicole A, Kather Jakob N, Pearson Alexander T
Pritzker School of Medicine, University of Chicago, Chicago, IL, United States.
Department of Medicine, University of Chicago, Chicago, IL, United States.
Front Oncol. 2021 Jun 8;11:630953. doi: 10.3389/fonc.2021.630953. eCollection 2021.
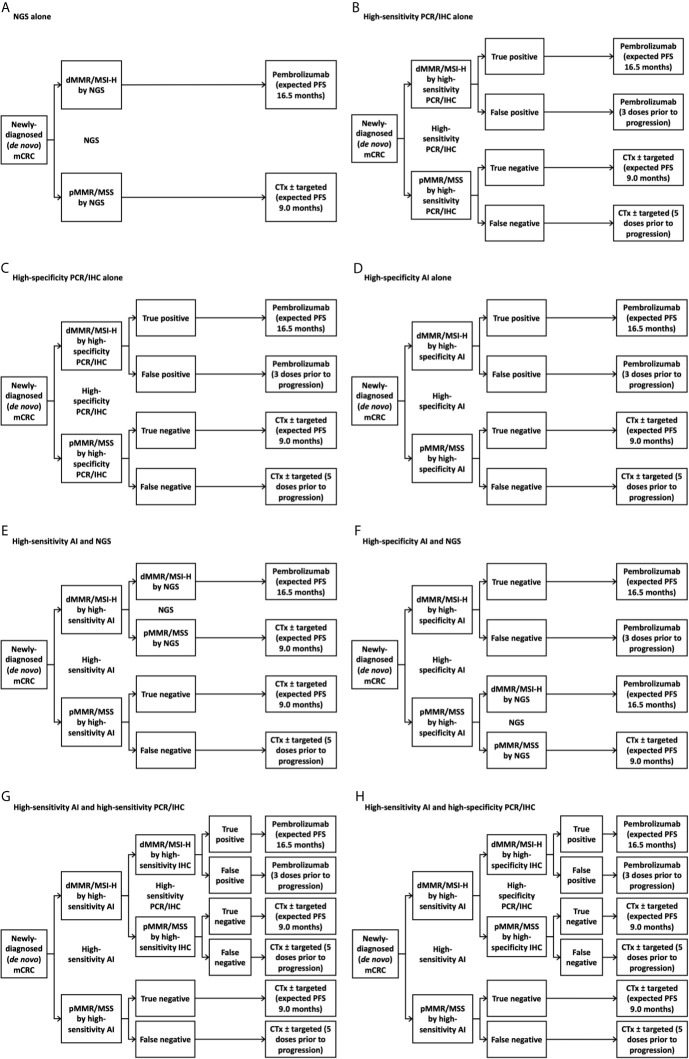
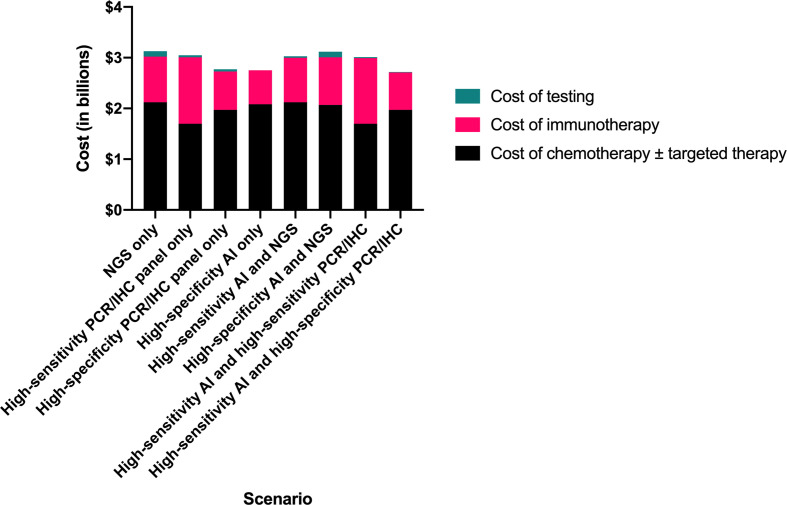
Rising cancer care costs impose financial burdens on health systems. Applying artificial intelligence to diagnostic algorithms may reduce testing costs and avoid wasteful therapy-related expenditures. To evaluate the financial and clinical impact of incorporating artificial intelligence-based determination of mismatch repair/microsatellite instability status into the first-line metastatic colorectal carcinoma setting, we developed a deterministic model to compare eight testing strategies: A) next-generation sequencing alone, B) high-sensitivity polymerase chain reaction or immunohistochemistry panel alone, C) high-specificity panel alone, D) high-specificity artificial intelligence alone, E) high-sensitivity artificial intelligence followed by next generation sequencing, F) high-specificity artificial intelligence followed by next-generation sequencing, G) high-sensitivity artificial intelligence and high-sensitivity panel, and H) high-sensitivity artificial intelligence and high-specificity panel. We used a hypothetical, nationally representative, population-based sample of individuals receiving first-line treatment for metastatic colorectal cancer (N = 32,549) in the United States. Model inputs were derived from secondary research (peer-reviewed literature and Medicare data). We estimated the population-level diagnostic costs and clinical implications for each testing strategy. The testing strategy that resulted in the greatest project cost savings (including testing and first-line drug cost) compared to next-generation sequencing alone in newly-diagnosed metastatic colorectal cancer was using high-sensitivity artificial intelligence followed by confirmatory high-specificity polymerase chain reaction or immunohistochemistry panel for patients testing negative by artificial intelligence ($400 million, 12.9%). The high-specificity artificial intelligence-only strategy resulted in the most favorable clinical impact, with 97% diagnostic accuracy in guiding genotype-directed treatment and average time to treatment initiation of less than one day. Artificial intelligence has the potential to reduce both time to treatment initiation and costs in the metastatic colorectal cancer setting without meaningfully sacrificing diagnostic accuracy. We expect the artificial intelligence value proposition to improve in coming years, with increasing diagnostic accuracy and decreasing costs of processing power. To extract maximal value from the technology, health systems should evaluate integrating diagnostic histopathologic artificial intelligence into institutional protocols, perhaps in place of other genotyping methodologies.
不断上涨的癌症治疗成本给卫生系统带来了经济负担。将人工智能应用于诊断算法可能会降低检测成本,并避免与治疗相关的浪费性支出。为了评估将基于人工智能的错配修复/微卫星不稳定性状态测定纳入一线转移性结直肠癌治疗的财务和临床影响,我们开发了一个确定性模型,以比较八种检测策略:A)仅进行下一代测序;B)仅进行高灵敏度聚合酶链反应或免疫组织化学检测;C)仅进行高特异性检测;D)仅进行高特异性人工智能检测;E)高灵敏度人工智能检测后进行下一代测序;F)高特异性人工智能检测后进行下一代测序;G)高灵敏度人工智能检测和高灵敏度检测;H)高灵敏度人工智能检测和高特异性检测。我们使用了一个假设的、具有全国代表性的、基于人群的样本,该样本来自美国接受一线转移性结直肠癌治疗的个体(N = 32,549)。模型输入数据来自二次研究(同行评审文献和医疗保险数据)。我们估计了每种检测策略的人群水平诊断成本和临床影响。与仅在新诊断的转移性结直肠癌中进行下一代测序相比,能带来最大项目成本节约(包括检测和一线药物成本)的检测策略是,对人工智能检测呈阴性的患者,先进行高灵敏度人工智能检测,然后进行确认性的高特异性聚合酶链反应或免疫组织化学检测(节省4亿美元,即12.9%)。仅采用高特异性人工智能的策略产生了最有利的临床影响,在指导基因型导向治疗方面诊断准确率为97%,平均治疗开始时间不到一天。在转移性结直肠癌治疗中,人工智能有潜力在不显著牺牲诊断准确率的情况下,缩短治疗开始时间并降低成本。我们预计,随着诊断准确率的提高和处理能力成本的降低,人工智能的价值主张将在未来几年得到改善。为了从该技术中获取最大价值,卫生系统应评估将诊断性组织病理学人工智能纳入机构方案,或许可以取代其他基因分型方法。