Department of Community Medicine and Rehabilitation, Unit of Geriatric Medicine, Umeå University, Umeå, Sweden; Department of Public Health and Clinical Medicine, Section of Sustainable Health, Umeå University, Umeå, Sweden.
Department of Community Medicine and Rehabilitation, Unit of Geriatric Medicine, Umeå University, Umeå, Sweden.
J Am Med Dir Assoc. 2021 Aug;22(8):1574-1580.e8. doi: 10.1016/j.jamda.2021.06.010. Epub 2021 Jun 24.
To compare 30-day mortality in long-term care facility (LTCF) residents with and without COVID-19 and to investigate the impact of 31 potential risk factors for mortality in COVID-19 cases.
Retrospective cohort study.
All residents of LTCFs registered in Senior Alert, a Swedish national database of health examinations in older adults, during 2019-2020.
We selected residents with confirmed COVID-19 until September 15, 2020, along with time-dependent propensity score-matched controls without COVID-19. Exposures were COVID-19, age, sex, comorbidities, medications, and other patient characteristics. The outcome was all-cause 30-day mortality.
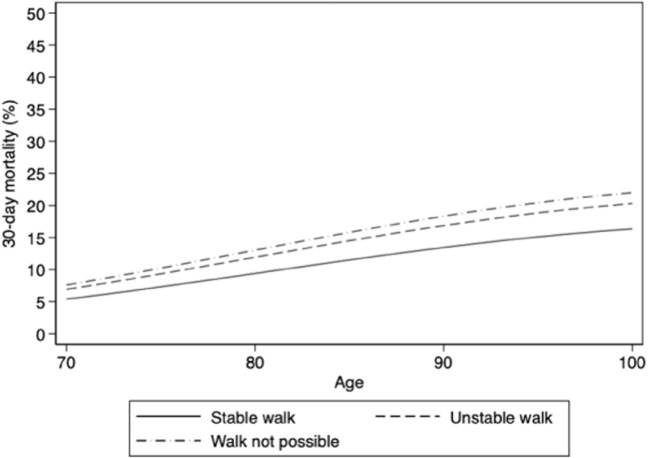
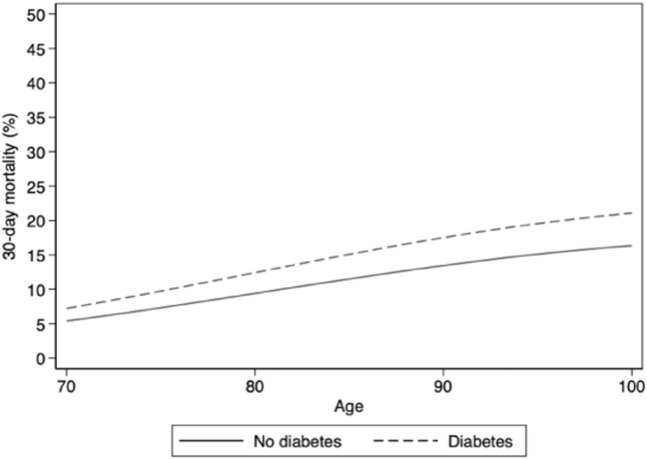
A total of 3731 residents (median age 87 years, 64.5% female) with COVID-19 were matched to 3731 controls without COVID-19. Thirty-day mortality was 39.9% in COVID-19 cases and 5.7% in controls [relative risk 7.05, 95% confidence interval (CI) 6.10-8.14]. In COVID-19 cases, the odds ratio (OR) for 30-day mortality was 2.44 (95% CI 1.57-3.81) in cases aged 80-84 years, 2.99 (95% CI 1.93-4.65) in cases aged 85-89 years, and 3.28 (95% CI 2.11-5.10) in cases aged ≥90 years, as compared with cases aged <70 years. Other risk factors for mortality among COVID-19 cases included male sex (OR, 2.60, 95% CI 2.22-3.05), neuropsychological conditions (OR, 2.18; 95% CI 1.76-2.71), impaired walking ability (OR, 1.45, 95% CI 1.17-1.78), urinary and bowel incontinence (OR 1.51, 95% CI 1.22-1.85), diabetes (OR 1.36, 95% CI 1.14-1.62), chronic kidney disease (OR 1.37, 95% CI 1.11-1.68) and previous pneumonia (OR 1.57, 95% CI 1.32-1.85). Nutritional factors, cardiovascular diseases, and antihypertensive medications were not significantly associated with mortality.
In Swedish LTCFs, COVID-19 was associated with a large excess in mortality after controlling for an extensive number of risk factors. Beyond older age and male sex, several prevalent clinical risk factors independently contributed to higher mortality. These findings suggest that reducing transmission of COVID-19 in LTCFs will likely prevent a considerable number of deaths.
比较有和无 COVID-19 的长期护理机构(LTCF)居民的 30 天死亡率,并调查 31 个可能导致 COVID-19 病例死亡的风险因素的影响。
回顾性队列研究。
2019-2020 年期间在瑞典老年人健康检查的全国数据库 Senior Alert 中登记的所有 LTCF 居民。
我们选择了截至 2020 年 9 月 15 日确诊 COVID-19 的居民,并与无 COVID-19 的时间依赖性倾向评分匹配对照进行了比较。暴露因素为 COVID-19、年龄、性别、合并症、药物和其他患者特征。结局是全因 30 天死亡率。
共纳入 3731 例(中位年龄 87 岁,64.5%为女性)COVID-19 患者,与 3731 例无 COVID-19 的对照相匹配。COVID-19 病例的 30 天死亡率为 39.9%,对照组为 5.7%[相对风险 7.05,95%置信区间(CI)6.10-8.14]。在 COVID-19 病例中,年龄 80-84 岁、85-89 岁和≥90 岁的病例与<70 岁的病例相比,30 天死亡率的比值比(OR)分别为 2.44(95%CI 1.57-3.81)、2.99(95%CI 1.93-4.65)和 3.28(95%CI 2.11-5.10)。COVID-19 病例死亡的其他危险因素包括男性(OR,2.60,95%CI 2.22-3.05)、神经心理状况(OR,2.18;95%CI 1.76-2.71)、行走能力受损(OR,1.45,95%CI 1.17-1.78)、尿便失禁(OR,1.51,95%CI 1.22-1.85)、糖尿病(OR,1.36,95%CI 1.14-1.62)、慢性肾脏病(OR,1.37,95%CI 1.11-1.68)和既往肺炎(OR,1.57,95%CI 1.32-1.85)。营养因素、心血管疾病和抗高血压药物与死亡率无显著相关性。
在瑞典的 LTCF 中,在控制了大量风险因素后,COVID-19 与死亡率的大幅增加相关。除了年龄较大和男性外,一些常见的临床危险因素也独立导致了更高的死亡率。这些发现表明,减少 COVID-19 在 LTCF 中的传播可能会预防相当数量的死亡。