MAP Centre for Urban Health Solutions, Li Ka Shing Knowledge Institute, St Michael's Hospital, 209 Victoria St, Toronto, ON, M5B 1T8, Canada.
Department of Psychiatry, University of Toronto, Toronto, ON, Canada.
J Urban Health. 2021 Aug;98(4):505-515. doi: 10.1007/s11524-021-00550-1. Epub 2021 Jun 28.
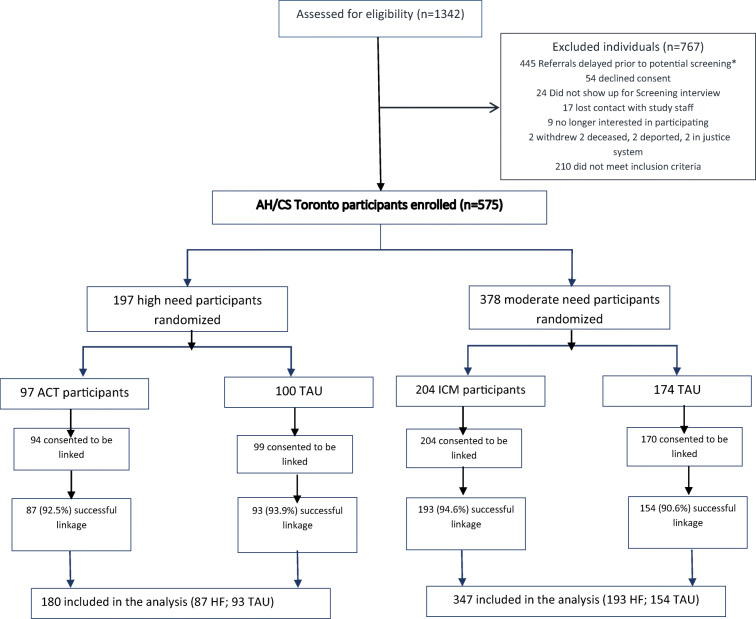
We assessed the effects of the Toronto Site Housing First (HF) intervention on hospitalizations and emergency department (ED) visits among homeless adults with mental illness over 7 years of follow-up. The Toronto Site is part of an unblinded multi-site randomized pragmatic trial of HF for homeless adults with mental illness in Canada, which followed participants up to 7 years. Five hundred seventy-five participants were recruited and classified as having high (HN) or moderate need (MN) for mental health support services. Each group was randomized into intervention (HF) and treatment as usual groups, and 567 (98.6%) consented to link their data to health administrative databases. HF participants received a monthly rent supplement of $600 (Canadian) and assertive community treatment (ACT) support or intensive care management (ICM) support based on need level. Treatment as usual (TAU) participants had access to social, housing, and health services generally available in the community. Outcomes included all-cause and mental health-specific hospitalization, number of days in hospital, and ED visit. We used GEE models to estimate ratio of rate ratios (RRR). The results showed HF with ACT had no significant effect on hospitalization rates among HN participants, but reduced the number of days in hospital (RRR = 0.32, 95% CI 0.16-0.63) and number of ED visits (RRR = 0.57, 95% CI 0.34-0.95). HF with ICM resulted in an increase in the number of hospitalizations (RRR = 1.69, 95% CI 1.09-2.60) and ED visit rates (RRR = 1.42, 95% CI 1.01-2.01) but had no effect in days in hospital for MN participants. Addressing the health needs of this population and reducing acute care utilization remain system priorities. Trial registration: http://www.isrctn.com/identifier: ISRCTN42520374.
我们评估了多伦多住房优先(HF)干预对 7 年随访期间患有精神疾病的无家可归成年人住院和急诊就诊的影响。多伦多站点是加拿大针对患有精神疾病的无家可归成年人的住房优先多站点、非盲、实用随机试验的一部分,该试验对参与者进行了长达 7 年的随访。共招募了 575 名参与者,并将其归类为具有较高(HN)或中等程度(MN)精神健康支持服务需求的患者。每个组都被随机分为干预(HF)和常规治疗组,其中 567 名(98.6%)同意将其数据与健康管理数据库链接。HF 参与者每月获得 600 加元(加拿大元)的租金补贴,并根据需求水平接受社区治疗(ACT)支持或强化护理管理(ICM)支持。常规治疗(TAU)参与者可以获得社区中通常提供的社会、住房和卫生服务。结果包括全因和精神健康特定的住院治疗、住院天数和急诊就诊次数。我们使用广义估计方程模型(GEE)来估计比率比(RRR)。结果表明,HF 联合 ACT 对 HN 参与者的住院率没有显著影响,但减少了住院天数(RRR=0.32,95%CI 0.16-0.63)和急诊就诊次数(RRR=0.57,95%CI 0.34-0.95)。HF 联合 ICM 增加了住院次数(RRR=1.69,95%CI 1.09-2.60)和急诊就诊率(RRR=1.42,95%CI 1.01-2.01),但对 MN 参与者的住院天数没有影响。满足这一人群的健康需求并减少急性护理的使用仍然是系统的重点。试验注册:http://www.isrctn.com/identifier:ISRCTN42520374。