Liggins Institute, The University of Auckland, Private Bag 92019, Auckland, New Zealand.
Liggins Institute, The University of Auckland, Private Bag 92019, Auckland, New Zealand; A Better Start - National Science Challenge, Auckland, New Zealand.
EBioMedicine. 2021 Jul;69:103443. doi: 10.1016/j.ebiom.2021.103443. Epub 2021 Jun 27.
Birth by caesarean section (CS) is associated with aberrant gut microbiome development and greater disease susceptibility later in life. We investigated whether oral administration of maternal vaginal microbiota to infants born by CS could restore their gut microbiome development in a pilot single-blinded, randomised placebo-controlled trial (Australian New Zealand Clinical Trials Registry, ACTRN12618000339257).
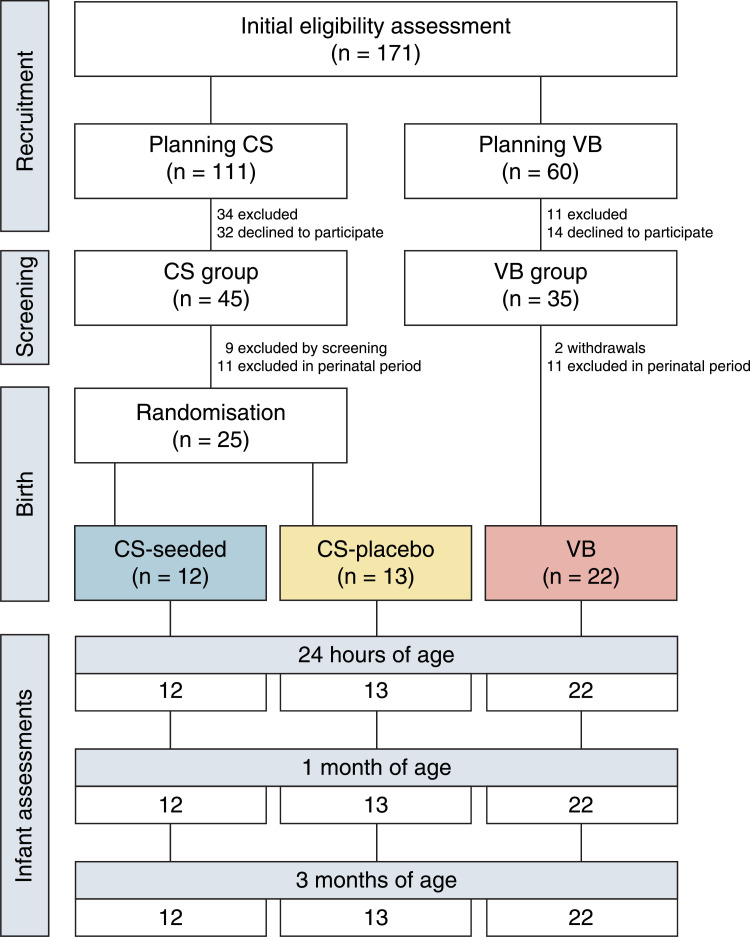
Pregnant women scheduled for a CS underwent comprehensive antenatal pathogen screening. At birth, healthy neonates were randomised to receive a 3 ml solution of either maternal vaginal microbes (CS-seeded, n = 12) or sterile water (CS-placebo, n = 13). Vaginally-born neonates were used as the reference control (VB, n = 22). Clinical assessments occurred within the first 2 h of birth, and at 1 month and 3 months of age. Infant stool samples and maternal vaginal extracts from CS women underwent shotgun metagenomic sequencing. The primary outcome was gut microbiome composition at 1 month of age. Secondary outcomes included maternal strain engraftment, functional potential of the gut microbiome, anthropometry, body composition, and adverse events.
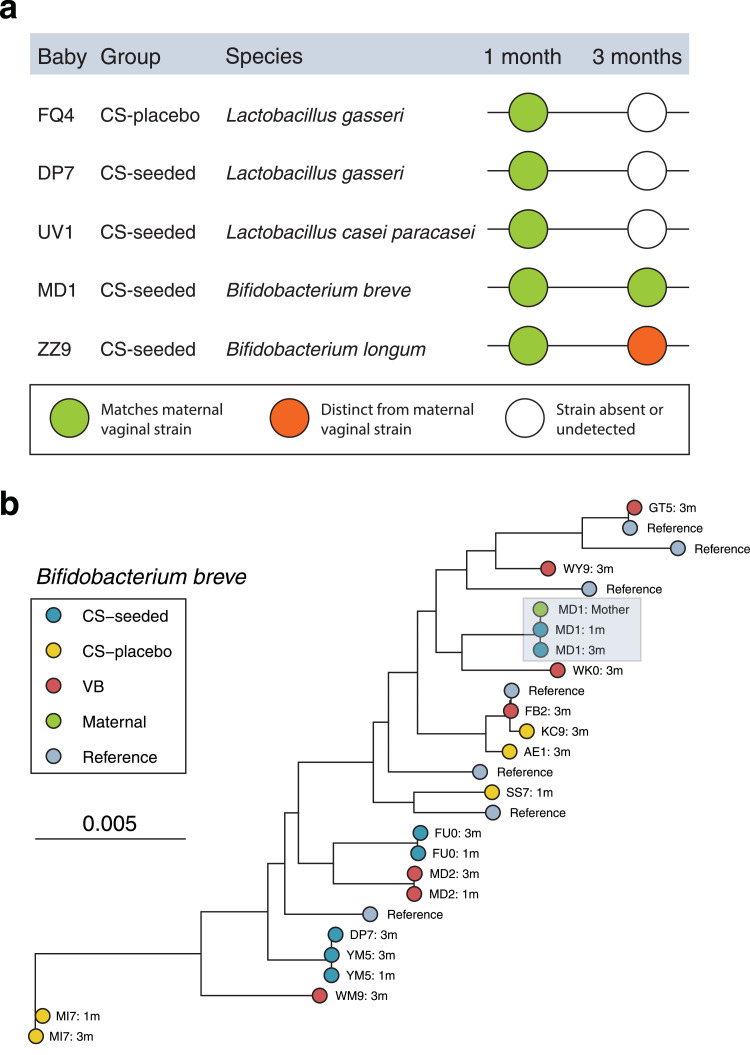
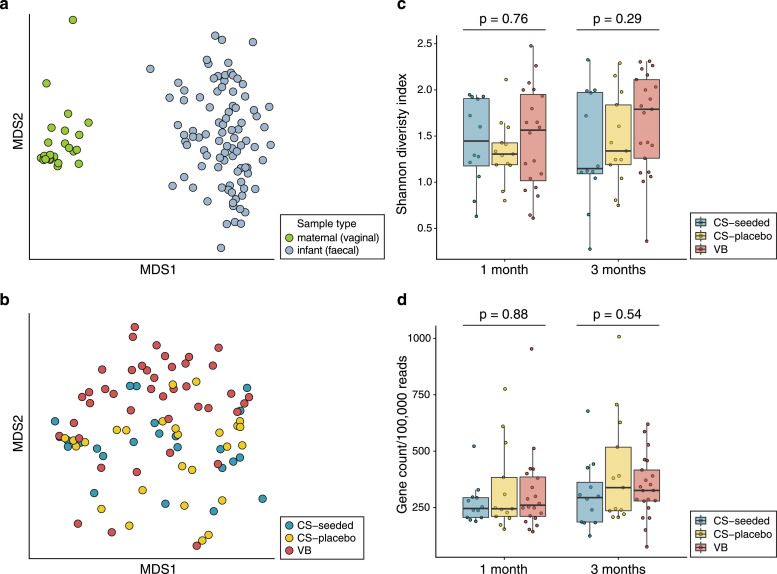
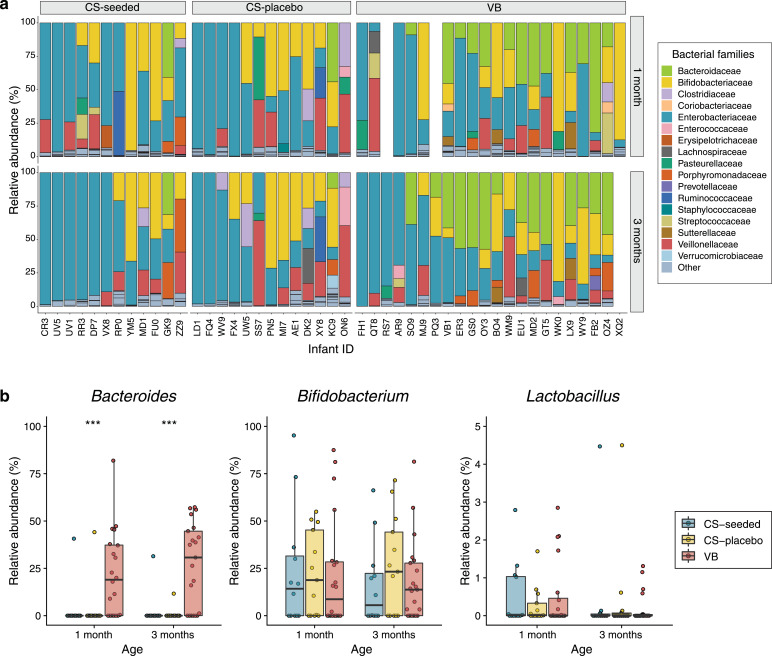
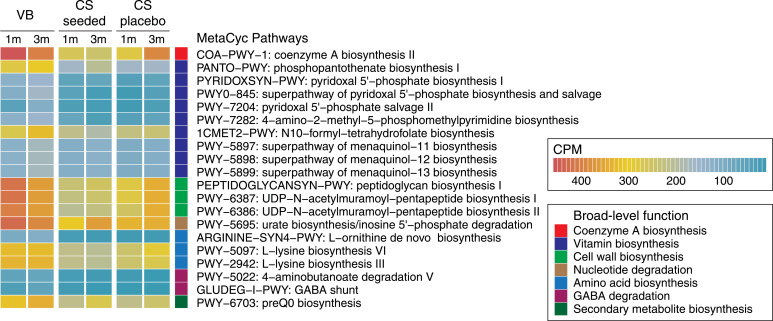
Despite the presence of viable microbial cells within transplant solutions, there were no observed differences in gut microbiome composition or functional potential between CS-seeded and CS-placebo infants at 1 month or 3 months of age. Both CS groups displayed the characteristic signature of low Bacteroides abundance, which contributed to a number of biosynthesis pathways being underrepresented when compared with VB microbiomes. Maternal vaginal strain engraftment was rare. Vaginal seeding had no observed effects on anthropometry or body composition. There were no serious adverse events associated with treatment.
Our pilot findings question the value of vaginal seeding given that oral administration of maternal vaginal microbiota did not alter early gut microbiome development in CS-born infants. The limited colonisation of maternal vaginal strains suggest that other maternal sources, such as the perianal area, may play a larger role in seeding the neonatal gut microbiome.
Health Research Council of New Zealand, A Better Start - National Science Challenge.
剖宫产(CS)会导致肠道微生物群落发育异常,并增加日后患病的易感性。我们通过一项单盲、随机、安慰剂对照的初步研究(澳大利亚和新西兰临床试验注册中心,ACTRN12618000339257),探究了 CS 分娩的婴儿经口摄入母体阴道微生物群能否恢复其肠道微生物群落的发育。
计划进行 CS 的孕妇接受全面的产前病原体筛查。新生儿出生时,将健康的新生儿随机分为接受 3 毫升母体阴道微生物(CS 定植组,n=12)或无菌水(CS 安慰剂组,n=13)的溶液。阴道分娩的新生儿作为参考对照(VB,n=22)。出生后 2 小时内进行临床评估,并在 1 个月和 3 个月时进行评估。婴儿粪便样本和 CS 产妇的阴道提取物进行鸟枪法宏基因组测序。主要结局是 1 个月时的肠道微生物群落组成。次要结局包括产妇定植菌株、肠道微生物群落的功能潜力、人体测量学、身体成分和不良事件。
尽管移植溶液中存在有活力的微生物细胞,但 CS 定植组和 CS 安慰剂组婴儿在 1 个月或 3 个月时的肠道微生物群落组成或功能潜力均无差异。两组 CS 婴儿均表现出低拟杆菌丰度的特征特征,与 VB 微生物组相比,许多生物合成途径的代表性不足。母体阴道定植菌株罕见。阴道定植对人体测量学或身体成分无明显影响。无与治疗相关的严重不良事件。
我们的初步研究结果对阴道定植的价值提出了质疑,因为口服母体阴道微生物群并没有改变 CS 分娩婴儿的早期肠道微生物群落发育。母体阴道菌株的定植有限表明,其他母体来源,如肛周区域,可能在定植新生儿肠道微生物群方面发挥更大的作用。
新西兰健康研究委员会,“更好的开始”——国家科学挑战。