Department of Epidemiology, Helmholtz Centre for Infection Research (HZI), Inhoffenstraße 7, 38124, Braunschweig, Germany.
PhD Programme Epidemiology, Helmholtz Centre for Infection Research (HZI), Inhoffenstraße 7, 38124, Braunschweig-Hannover, Germany.
Syst Rev. 2021 Jun 30;10(1):194. doi: 10.1186/s13643-021-01732-3.
Comprehensive evidence synthesis on the associations between comorbidities and behavioural factors with hospitalisation, intensive care unit (ICU) admission, and death due to COVID-19 is required for deriving national and international recommendations on primary targets for non-pharmacological interventions (NPI) and vaccination strategies.
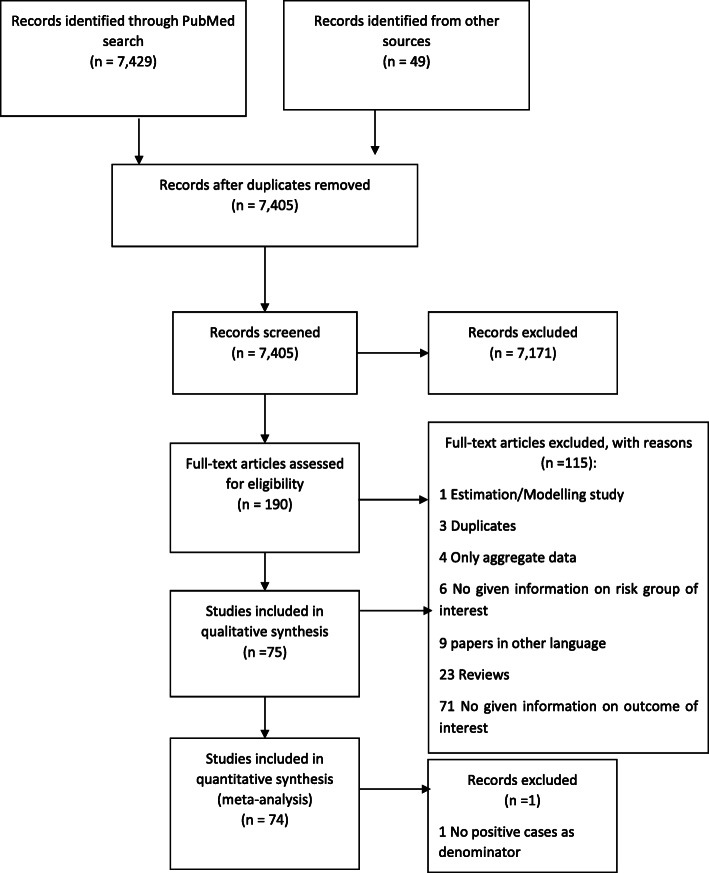
We performed a rapid systematic review and meta-analysis on studies and publicly accessible data to quantify associations between predisposing health conditions, demographics, behavioural factors on the one hand and hospitalisation, ICU admission, and death from COVID-19 on the other hand. We provide ranges of reported and calculated effect estimates and pooled relative risks derived from a meta-analysis and meta-regression.
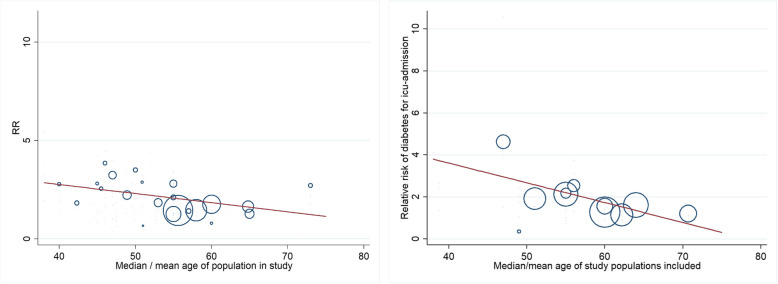
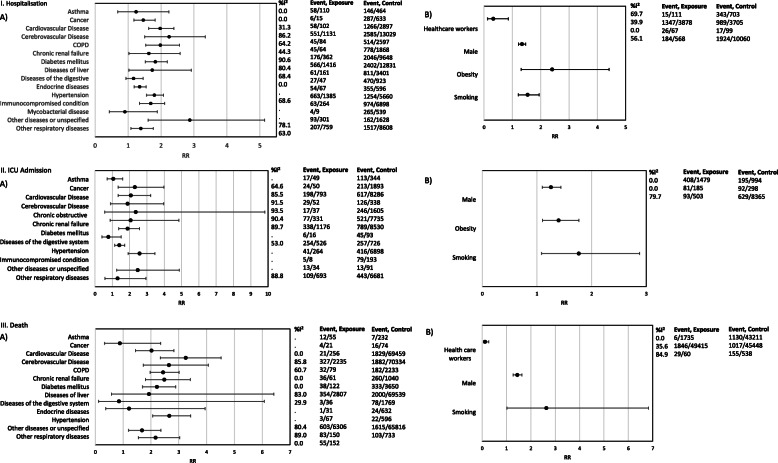
Seventy-five studies were included in qualitative and 74 in quantitative synthesis, with study populations ranging from 19 to 44,672 COVID-19 cases. The risk of dying from COVID-19 was significantly associated with cerebrovascular [pooled relative risk (RR) 2.7 (95% CI 1.7-4.1)] and cardiovascular [RR 3.2 (CI 2.3-4.5)] diseases, hypertension [RR 2.6 (CI 2.0-3.4)], and renal disease [RR 2.5 (CI 1.8-3.4)], with high heterogeneity in pooled estimates, partly but not solely explained by age of study participants. For some comorbidities, our meta-regression showed a decrease in effect on the severity of disease with a higher median age of the study population. Compared to death, associations between several comorbidities and hospitalisation and ICU admission were less pronounced.
We obtained robust estimates on the magnitude of risk for COVID-19 hospitalisation, ICU admission, and death associated with comorbidities, demographic, and behavioural risk factors and show that these estimates are modified by age of study participants. This interaction is an important finding to be kept in mind for current vaccination strategies and for the protection of individuals with high risk for a severe COVID-19 course.
为了制定国家和国际建议,确定非药物干预(NPI)和疫苗接种策略的主要目标,需要综合评估合并症和行为因素与 COVID-19 住院、重症监护病房(ICU)入院和死亡之间的关联。
我们对研究和公开可获得的数据进行了快速系统评价和荟萃分析,以量化先天健康状况、人口统计学和行为因素与 COVID-19 住院、ICU 入院和死亡之间的关联。我们提供了来自荟萃分析和荟萃回归的报告和计算的效应估计值和合并相对风险的范围。
75 项研究纳入定性综合分析,74 项研究纳入定量综合分析,研究人群范围从 19 例至 44672 例 COVID-19 病例。死于 COVID-19 的风险与脑血管疾病(合并相对风险[RR]2.7[95%置信区间[CI]1.7-4.1])和心血管疾病(RR 3.2[CI 2.3-4.5])、高血压(RR 2.6[CI 2.0-3.4])和肾脏疾病(RR 2.5[CI 1.8-3.4])显著相关,合并估计值存在高度异质性,部分但不完全由研究参与者的年龄解释。对于某些合并症,我们的荟萃回归显示,随着研究人群的平均年龄增加,疾病严重程度的影响降低。与死亡相比,几种合并症与住院和 ICU 入院的关联程度较低。
我们获得了与合并症、人口统计学和行为危险因素相关的 COVID-19 住院、ICU 入院和死亡风险的稳健估计值,并表明这些估计值受研究参与者年龄的影响。这种相互作用是当前疫苗接种策略和保护高风险 COVID-19 严重程度个体时需要牢记的重要发现。