Department of Hepatopancreatobiliary Surgery, Ningbo Medical Centre Lihuili Hospital, Ningbo University, Ningbo, 315040, Zhejiang, China.
Sci Rep. 2021 Jul 7;11(1):13999. doi: 10.1038/s41598-021-93528-7.
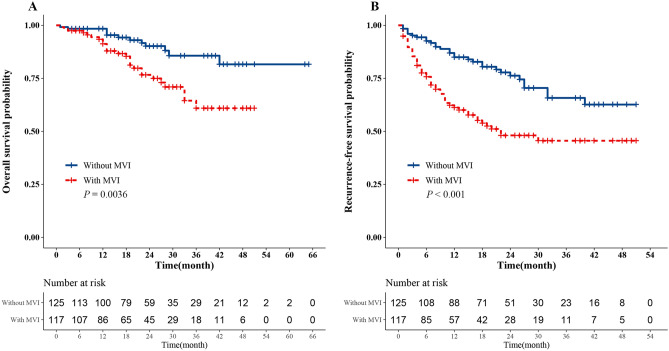
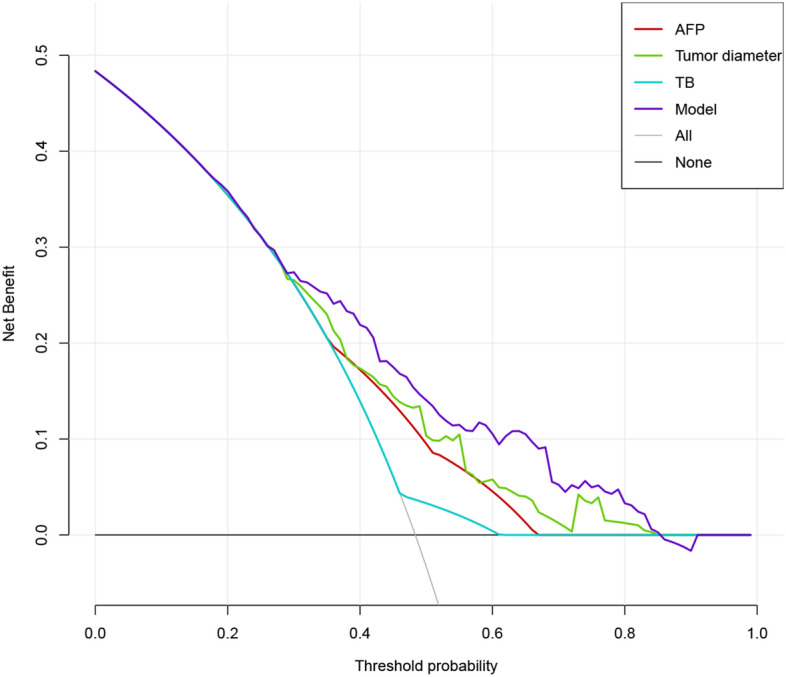
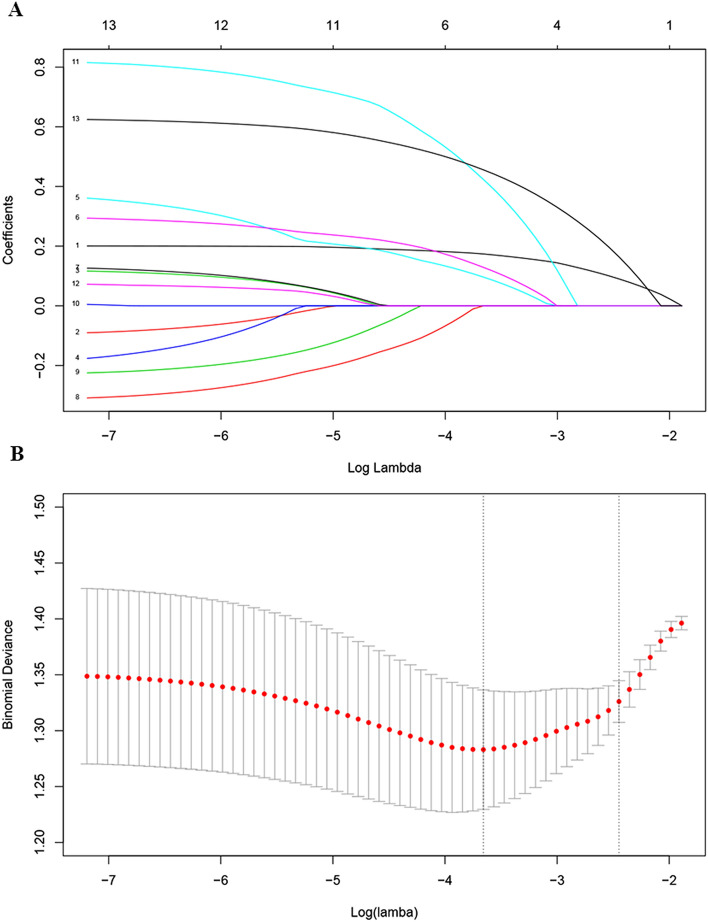
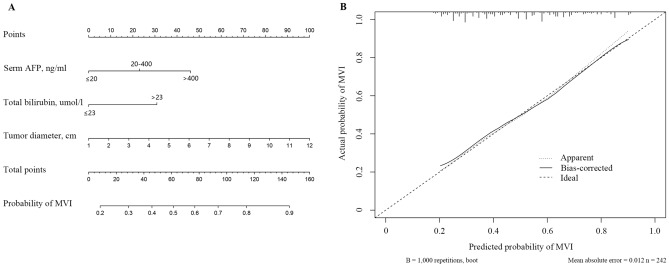
The presence of microvascular invasion (MVI) is a critical determinant of early hepatocellular carcinoma (HCC) recurrence and prognosis. We developed a nomogram model integrating clinical laboratory examinations and radiological imaging results from our clinical database to predict microvascular invasion presence at preoperation in HCC patients. 242 patients with pathologically confirmed HCC at the Ningbo Medical Centre Lihuili Hospital from September 2015 to January 2021 were included in this study. Baseline clinical laboratory examinations and radiological imaging results were collected from our clinical database. LASSO regression analysis model was used to construct data dimensionality reduction and elements selection. Multivariate logistic regression analysis was performed to identify the independent risk factors associated with MVI and finally a nomogram for predicting MVI presence of HCC was established. Nomogram performance was assessed via internal validation and calibration curve statistics. Decision curve analysis (DCA) was conducted to determine the clinical usefulness of the nomogram model by quantifying the net benefits along with the increase in threshold probabilities. Survival analysis indicated that the probability of overall survival (OS) and recurrence-free survival (RFS) were significantly different between patients with MVI and without MVI (P < 0.05). Histopathologically identified MVI was found in 117 of 242 patients (48.3%). The preoperative factors associated with MVI were large tumor diameter (OR = 1.271, 95%CI: 1.137-1.420, P < 0.001), AFP level greater than 20 ng/mL (20-400 vs. ≤ 20, OR = 2.025, 95%CI: 1.056-3.885, P = 0.034; > 400 vs. ≤ 20, OR = 3.281, 95%CI: 1.661-6.480, P = 0.001), total bilirubin level greater than 23 umol/l (OR = 2.247, 95%CI: 1.037-4.868, P = 0.040). Incorporating tumor diameter, AFP and TB, the nomogram achieved a better concordance index of 0.725 (95%CI: 0.661-0.788) in predicting MVI presence. Nomogram analysis showed that the total factor score ranged from 0 to 160, and the corresponding risk rate ranged from 0.20 to 0.90. The DCA showed that if the threshold probability was > 5%, using the nomogram to diagnose MVI could acquire much more benefit. And the net benefit of the nomogram model was higher than single variable within 0.3-0.8 of threshold probability. In summary, the presence of MVI is an independent prognostic risk factor for RFS. The nomogram detailed here can preoperatively predict MVI presence in HCC patients. Using the nomogram model may constitute a usefully clinical tool to guide a rational and personalized subsequent therapeutic choice.
微血管侵犯(MVI)的存在是肝细胞癌(HCC)早期复发和预后的关键决定因素。我们从临床数据库中整合了临床实验室检查和影像学结果,开发了一个列线图模型,以预测 HCC 患者术前 MVI 的存在。本研究纳入了 2015 年 9 月至 2021 年 1 月在宁波医疗中心李惠利医院经病理证实的 242 例 HCC 患者。从临床数据库中收集了基线临床实验室检查和影像学结果。使用 LASSO 回归分析模型进行数据降维和元素选择。多变量 logistic 回归分析用于确定与 MVI 相关的独立危险因素,最终建立了预测 HCC 患者 MVI 存在的列线图。通过内部验证和校准曲线统计来评估列线图的性能。决策曲线分析(DCA)通过量化随着阈值概率增加的净效益,来确定列线图模型的临床实用性。生存分析表明,MVI 阳性和阴性患者的总生存(OS)和无复发生存(RFS)概率差异有统计学意义(P<0.05)。在 242 例患者中,有 117 例(48.3%)组织病理学上发现 MVI。与 MVI 相关的术前因素包括肿瘤直径较大(OR=1.271,95%CI:1.137-1.420,P<0.001)、AFP 水平大于 20ng/ml(20-400 与≤20ng/ml,OR=2.025,95%CI:1.056-3.885,P=0.034;>400 与≤20ng/ml,OR=3.281,95%CI:1.661-6.480,P=0.001)、总胆红素水平大于 23μmol/L(OR=2.247,95%CI:1.037-4.868,P=0.040)。纳入肿瘤直径、AFP 和 TB 后,列线图在预测 MVI 存在方面的一致性指数为 0.725(95%CI:0.661-0.788)。列线图分析显示,总积分范围为 0 至 160,相应的风险率范围为 0.20 至 0.90。DCA 表明,如果阈值概率>5%,使用列线图诊断 MVI 可获得更多益处。并且,在 0.3-0.8 阈值概率范围内,列线图模型的净效益高于单一变量。综上所述,MVI 的存在是 RFS 的一个独立预后危险因素。本研究详细描述的列线图可术前预测 HCC 患者的 MVI 存在。使用列线图模型可能构成一种有用的临床工具,以指导合理和个性化的后续治疗选择。