National Institute for Viral Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, China.
Emergency Department of COVID-19, Beijing Ditan Hospital, Capital Medical University, Beijing, China.
Microbiol Spectr. 2021 Sep 3;9(1):e0027321. doi: 10.1128/Spectrum.00273-21. Epub 2021 Aug 4.
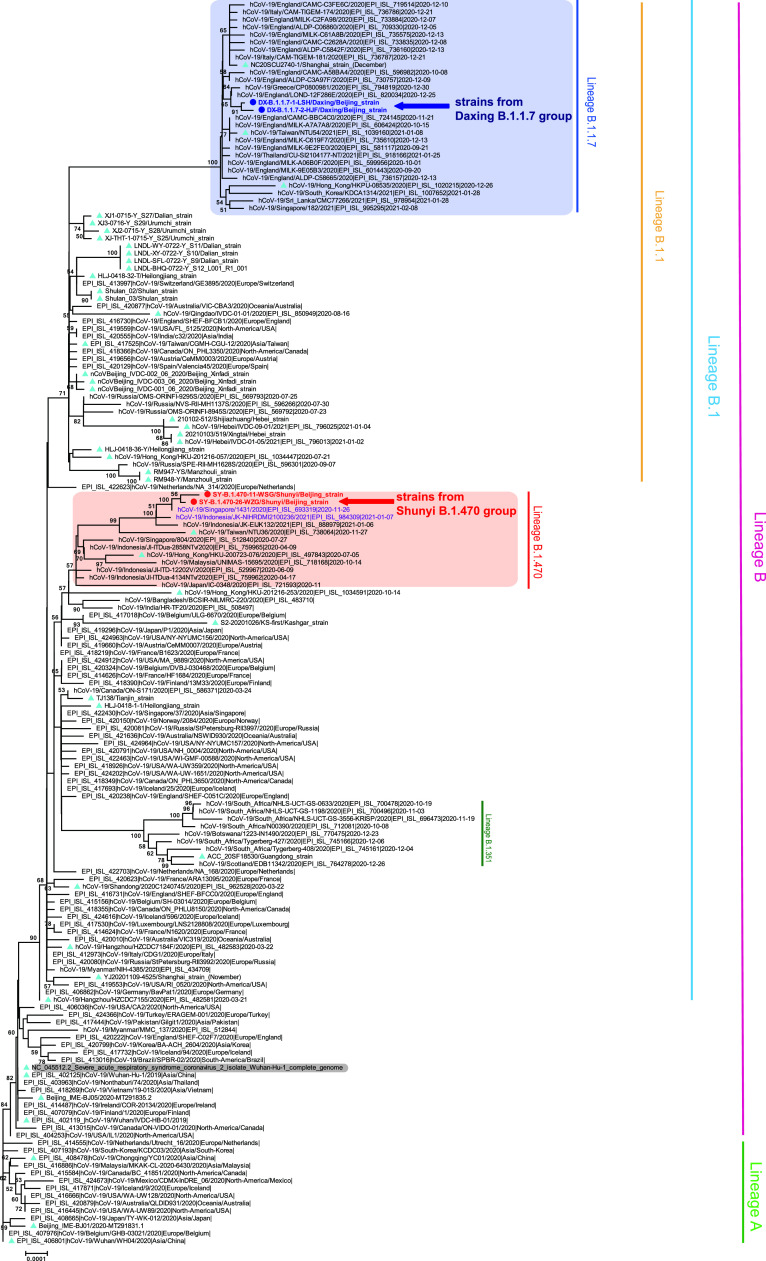
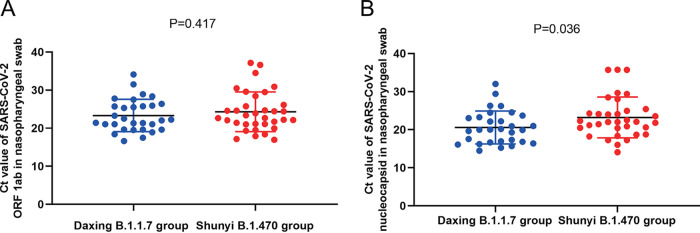
The SARS-CoV-2 B.1.1.7 variant has increased sharply in numbers worldwide and is reported to be more contagious than the nonvariant. Little is known regarding the detailed clinical features of B.1.1.7 variant infection. Data on 74 COVID-19 cases from two outbreaks in two districts of Beijing, China were extracted from a cloud database, including 41 cases from Shunyi District (Shunyi B.1.470 group) and 33 from Daxing (Daxing B.1.1.7 group) from December 25, 2020 to January 17, 2021. We conducted a comparison of the clinical characteristics. Seven clinical indicators of the Daxing B.1.1.7 group were significantly higher than those of the Shunyi group, including the proportion with fever over 38°C, the levels of C-reactive protein (CRP), serum amyloid A (SAA), creatine kinase (CK), d-dimer (DD), and CD4 T lymphocytes (CD4 T), and the proportion with ground-glass opacity (GGO) in the lung ( values of ≤0.05). After adjusting for age, B.1.1.7 variant infection was a risk factor for elevated CRP ( = 0·045), SAA ( = 0·011), CK ( = 0·034), and CD4 T ( = 0.029) and for the presence of GGO ( = 0.005). The median threshold cycle () value of reverse transcriptase quantitative PCR (RT-qPCR) tests of the N gene target in the Daxing B.1.1.7 group was significantly lower ( = 0.036) than that in the Shunyi B.1.470 group. Clinical features, including a more serious inflammatory response, pneumonia, and a possibly higher viral load, were detected in the cases infected with B.1.1.7 SARS-CoV-2. The B.1.1.7 variant may have increased pathogenicity. The SARS-CoV-2 B.1.1.7 variant, which was first identified in the United Kingdom, has increased sharply in numbers worldwide and was reported to be more contagious than the nonvariant. To our knowledge, no studies investigating the detailed clinical features of COVID-19 cases infected with the B.1.1.7 variant have been published. Local epidemics have rarely occurred in China, but occasionally, a small clustered outbreak triggered by an imported SARS-CoV-2 strain with only one chain of transmission could happen. From late 2020 to early 2021, two clustered COVID-19 outbreaks occurred in Beijing, one of which was caused by the B.1.1.7 variant. The COVID-19 patients from the two outbreaks received similar clinical tests, diagnoses, and treatments. We found that the B.1.1.7 variant infection could lead to a more serious inflammatory response, acute response process, more severe pneumonia, and probably higher viral loads. This therefore implies that the B.1.1.7 variant may have increased pathogenicity.
新冠病毒 B.1.1.7 变异株在全球范围内数量急剧增加,据报道其传染性高于非变异株。关于 B.1.1.7 变异株感染的详细临床特征知之甚少。我们从一个云端数据库中提取了 2020 年 12 月 25 日至 2021 年 1 月 17 日期间发生在北京两个区(顺义区,顺义 B.1.470 组;大兴区,大兴 B.1.1.7 组)的两起疫情中的 74 例 COVID-19 病例数据,包括 41 例来自顺义区(顺义 B.1.470 组)和 33 例来自大兴区(大兴 B.1.1.7 组)。我们对这些临床特征进行了比较。与顺义组相比,大兴 B.1.1.7 组的 7 个临床指标明显升高,包括发热超过 38°C 的比例、C 反应蛋白(CRP)、血清淀粉样蛋白 A(SAA)、肌酸激酶(CK)、D-二聚体(DD)和 CD4 淋巴细胞(CD4 T)的水平,以及肺部磨玻璃密度影(GGO)的比例( 值≤0.05)。在调整年龄后,B.1.1.7 变异株感染是 CRP( = 0·045)、SAA( = 0·011)、CK( = 0·034)和 CD4 T( = 0.029)升高和 GGO( = 0.005)的危险因素。大兴 B.1.1.7 组中 N 基因靶标逆转录酶定量 PCR(RT-qPCR)检测的中位阈值循环( )值明显低于顺义 B.1.470 组( = 0.036)。在感染 B.1.1.7 SARS-CoV-2 的病例中,我们检测到更严重的炎症反应、肺炎和可能更高的病毒载量等临床特征。B.1.1.7 变异株可能具有更高的致病性。
首先在英国发现的新冠病毒 B.1.1.7 变异株在全球范围内数量急剧增加,据报道其传染性高于非变异株。据我们所知,目前尚无关于感染 B.1.1.7 变异株的 COVID-19 病例详细临床特征的研究。中国很少发生局部疫情,但偶尔也会发生由单一传播链的输入性 SARS-CoV-2 株引起的小范围聚集性疫情。2020 年末至 2021 年初,北京发生了两起聚集性 COVID-19 疫情,其中一起是由 B.1.1.7 变异株引起的。两起疫情中的 COVID-19 患者接受了相似的临床检查、诊断和治疗。我们发现,B.1.1.7 变异株感染可能导致更严重的炎症反应、急性反应过程、更严重的肺炎和可能更高的病毒载量。这表明 B.1.1.7 变异株可能具有更高的致病性。