Department of Public Health, Erasmus MC University Medical Center, Na-building, room Na-2318, Wytemaweg 80, 3015, Rotterdam, CN, The Netherlands.
Trauma Research Unit, Department of Surgery, Erasmus MC University Medical Center, Na-building, room Na-2318, Wytemaweg 80, 3015, Rotterdam, CN, The Netherlands.
BMC Emerg Med. 2021 Aug 6;21(1):93. doi: 10.1186/s12873-021-00487-3.
Prehospital triage protocols typically try to select patients with Injury Severity Score (ISS) above 15 for direct transportation to a Level-1 trauma center. However, ISS does not necessarily discriminate between patients who benefit from immediate care at Level-1 trauma centers. The aim of this study was to assess which patients benefit from direct transportation to Level-1 trauma centers.
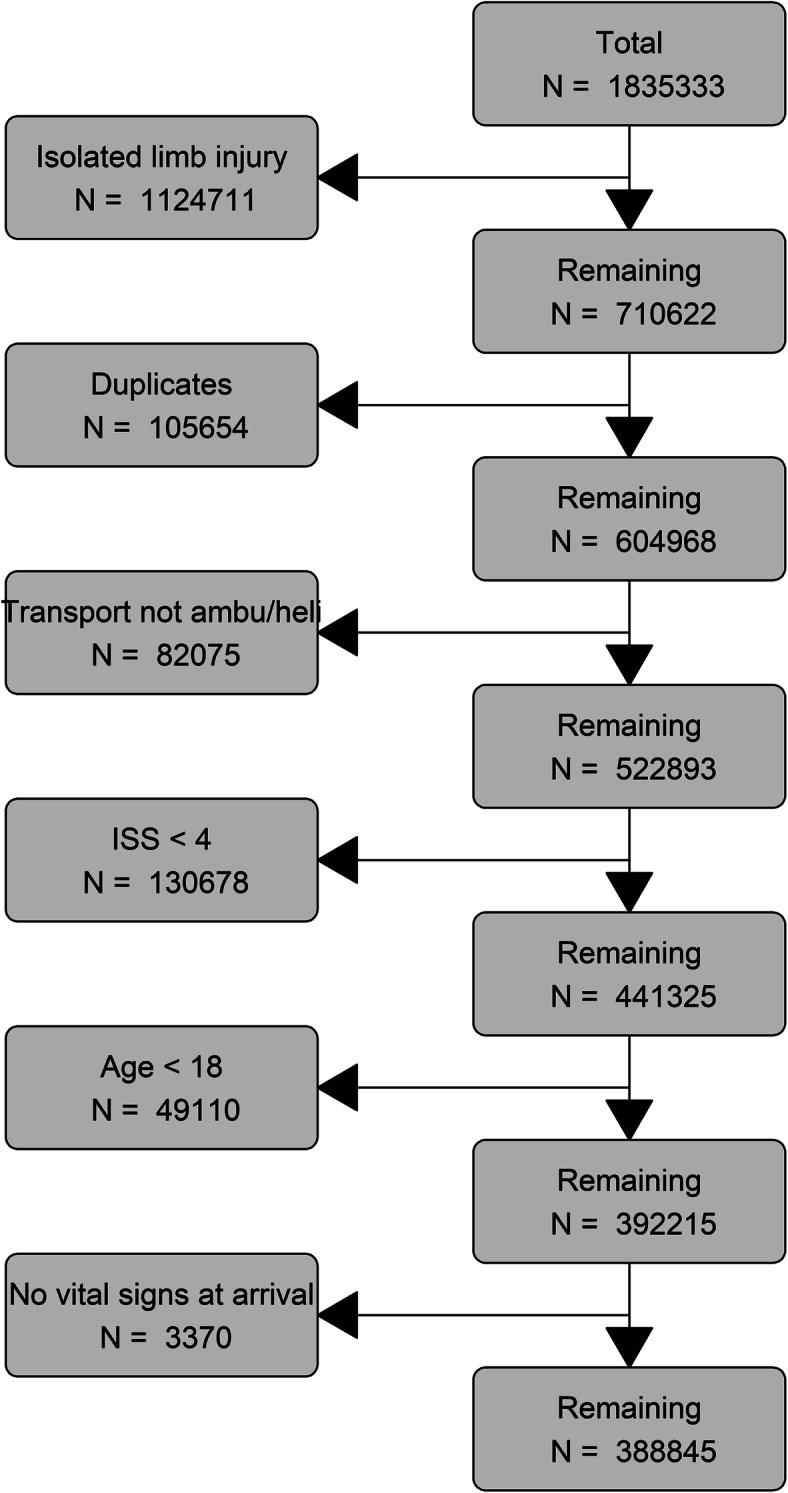
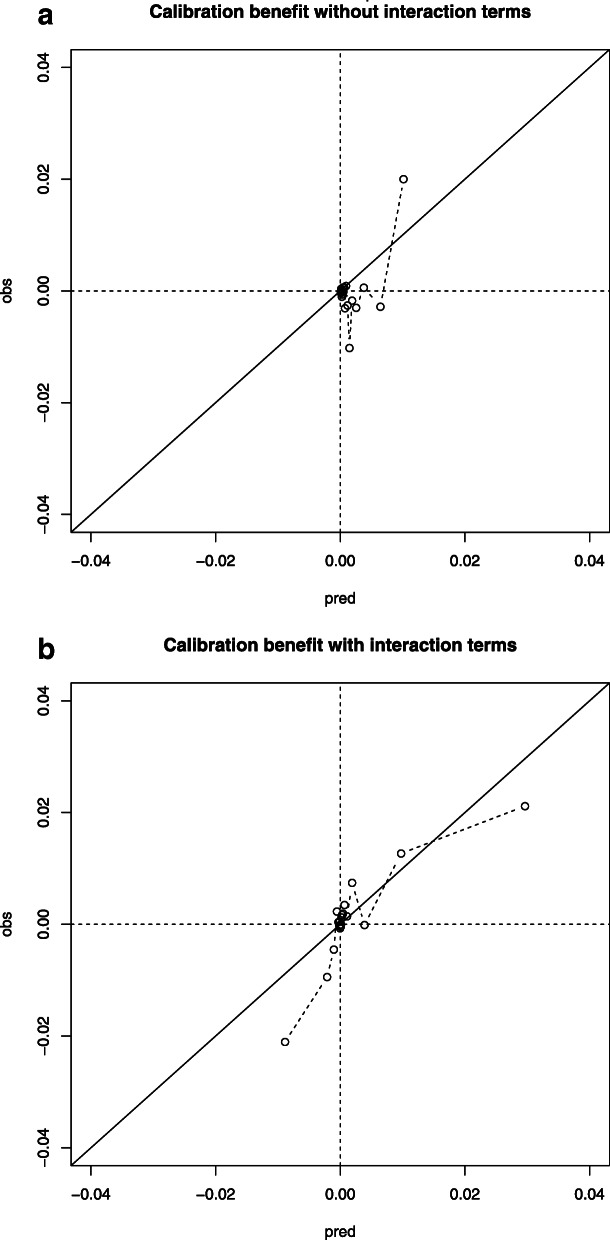
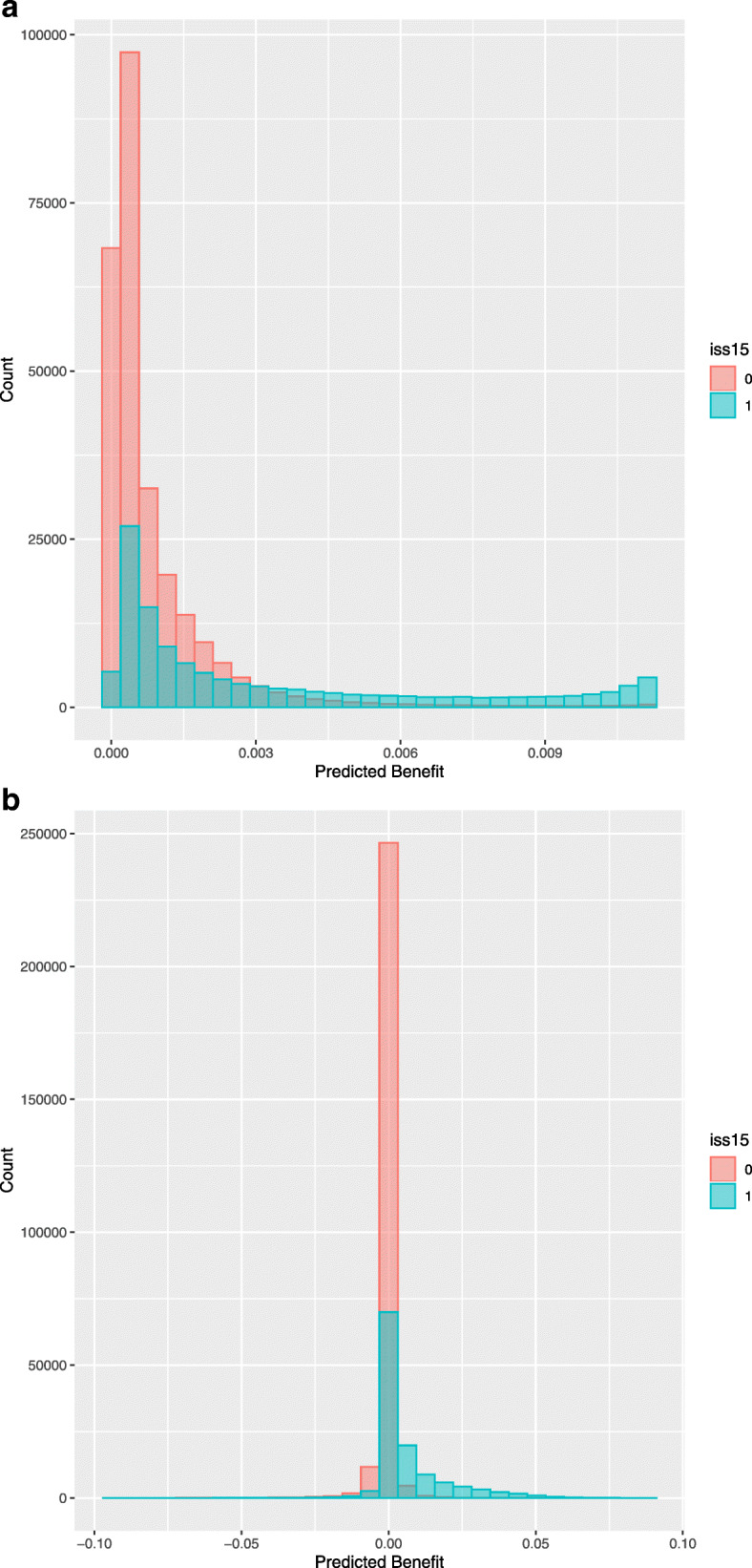
We used the American National Trauma Data Bank (NTDB), a retrospective observational cohort. All adult patients (ISS > 3) between 2015 and 2016 were included. Patients who were self-presenting or had isolated limb injury were excluded. We used logistic regression to assess the association of direct transportation to Level-1 trauma centers with in-hospital mortality adjusted for clinically relevant confounders. We used this model to define benefit as predicted probability of mortality associated with transportation to a non-Level-1 trauma center minus predicted probability associated with transportation to a Level-1 trauma center. We used a threshold of 1% as absolute benefit. Potential interaction terms with transportation to Level-1 trauma centers were included in a penalized logistic regression model to study which patients benefit.
We included 388,845 trauma patients from 232 Level-1 centers and 429 Level-2/3 centers. A small beneficial effect was found for direct transportation to Level-1 trauma centers (adjusted Odds Ratio: 0.96, 95% Confidence Interval: 0.92-0.99) which disappeared when comparing Level-1 and 2 versus Level-3 trauma centers. In the risk approach, predicted benefit ranged between 0 and 1%. When allowing for interactions, 7% of the patients (n = 27,753) had more than 1% absolute benefit from direct transportation to Level-1 trauma centers. These patients had higher AIS Head and Thorax scores, lower GCS and lower SBP. A quarter of the patients with ISS > 15 were predicted to benefit from transportation to Level-1 centers (n = 26,522, 22%).
Benefit of transportation to a Level-1 trauma centers is quite heterogeneous across patients and the difference between Level-1 and Level-2 trauma centers is small. In particular, patients with head injury and signs of shock may benefit from care in a Level-1 trauma center. Future prehospital triage models should incorporate more complete risk profiles.
院前分诊方案通常试图选择损伤严重程度评分(ISS)高于 15 的患者直接送往一级创伤中心。然而,ISS 并不能区分哪些患者从一级创伤中心的即时治疗中获益。本研究旨在评估哪些患者从直接送往一级创伤中心获益。
我们使用美国国家创伤数据库(NTDB),这是一个回顾性观察队列。纳入 2015 年至 2016 年间所有 ISS 大于 3 的成年患者。排除自行就诊或仅有肢体损伤的患者。我们使用逻辑回归评估直接送往一级创伤中心与院内死亡率之间的关联,调整了临床相关混杂因素。我们使用该模型定义获益为与送往非一级创伤中心相关的死亡率预测值减去与送往一级创伤中心相关的死亡率预测值。我们使用 1%的绝对获益作为阈值。在惩罚逻辑回归模型中纳入与送往一级创伤中心相关的潜在交互项,以研究哪些患者获益。
我们纳入了来自 232 个一级中心和 429 个二级/三级中心的 388845 名创伤患者。直接送往一级创伤中心有较小的获益效应(调整后的优势比:0.96,95%置信区间:0.92-0.99),而与一级和二级创伤中心相比,一级和三级创伤中心之间的差异消失。在风险方法中,预测获益范围在 0 到 1%之间。当允许交互作用时,7%的患者(n=27753)从直接送往一级创伤中心的治疗中获益超过 1%。这些患者的 AIS 头部和胸部评分较高,GCS 和 SBP 较低。ISS 大于 15 的患者中有四分之一预计从送往一级中心的治疗中获益(n=26522,22%)。
送往一级创伤中心的获益在患者之间差异较大,一级和二级创伤中心之间的差异较小。特别是头部受伤和休克迹象的患者可能从一级创伤中心的治疗中获益。未来的院前分诊模型应纳入更完整的风险概况。